Department of Epidemiology and Biostatistics, School of Public Health, Xi'an Jiaotong University Health Science Center, No 76 West Yanta Road, Xi'an, 710061, Shaanxi Province, People's Republic of China.
Department of Epidemiology and Biostatistics, Asmara College of Health Sciences, School of Public Health, P.O.Box 8566, Asmara, Eritrea.
BMC Public Health. 2020 Jan 6;20(1):10. doi: 10.1186/s12889-019-8118-x.
Limited knowledge on the magnitude of neonatal mortality and associated factors is hampering early intervention in African countries.
To determine neonatal mortality and associated factors in the Specialized Neonatal Care Unit Asmara, Eritrea.
Medical records of all neonates admitted to the Specialized Neonatal Care Unit in 2016 were reviewed using a cross-sectional study. The most important causes of admission and mortality were analyzed. Univariate and multivariate logistic regression analysis was used to evaluate the strength of risk factors associated with neonatal mortality. Variables significant at P < 0.20 level in the univariate analysis were retained in the multivariate model. Model fit was evaluated using Hosmer and Lemeshow test (Chi-square = 12.89, df = 8; P = 0.116), implies the model's estimates fit the data at an acceptable level. Collinearity was assessed using variance inflation factor (VIF) < 4. P-value < 0.05 was considered statistically significant.
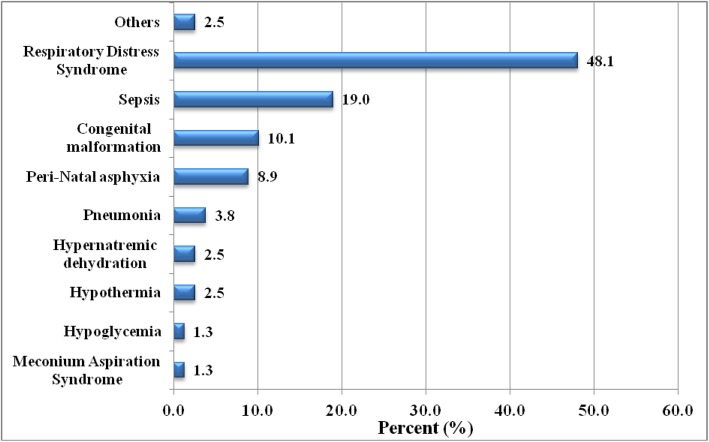
Of the 1204 (59.9% boys and 40.1% girls) neonates admitted in 2016, 79 (65.6/1000 live births) died. The major causes of admission were sepsis (35.5%), respiratory distress syndrome (15.4%) and perinatal asphyxia (10%). Major causes of death were respiratory distress syndrome (48.1%); extremely low birth weight (40.9%) and very low birth weight (30.5%). After adjustment, low birth weight (Adjusted odds ratio (AOR) = 4.55, 95% CI,1.97-10.50), very low birth weight (AOR = 19.24, 95% CI, 5.80-63.78), late admission (24 h after diagnosis) (AOR = 2.96, 95% CI, 1.34-6.52), apgar score (in 1 min AOR = 2.28, 95% CI, 1.09-4.76, in 5 min AOR = 2.07, 95% CI, 1.02-4.22), and congenital abnormalities (AOR = 3.95, 95% CI, 1.59-9.85) were significantly associated with neonatal mortality. Neonates that stayed > 24 h in the Specialized Neonatal Care Unit (AOR = 0.23, 95% CI, 0.11-0.46) had a lower likelihood of death. Overall 95.8% of mothers of neonates attended antenatal care and 96.6% were facility delivered. None of the maternal conditions were associated with neonatal mortality in this study.
Low birth weight, late admission, low apgar scores and congenital abnormalities were significantly associated with neonatal mortality in the Specialized Neonatal Care Unit. Early management of low birth weight, preterm births, and neonatal complications should be the priority issues for controlling local neonatal deaths.
在非洲国家,由于对新生儿死亡率及其相关因素的了解有限,早期干预措施受到阻碍。
确定厄立特里亚阿斯马拉专科新生儿护理病房的新生儿死亡率及其相关因素。
采用横断面研究方法,对 2016 年入住专科新生儿护理病房的所有新生儿的病历进行回顾性分析。分析主要入院原因和死亡原因。采用单因素和多因素逻辑回归分析评估与新生儿死亡率相关的危险因素的强度。单因素分析中 P 值<0.20 的变量被保留在多因素模型中。采用 Hosmer 和 Lemeshow 检验(卡方=12.89,df=8;P=0.116)评估模型拟合度(表示模型的估计值在可接受的水平上与数据拟合)。使用方差膨胀因子(VIF)<4 评估共线性。P 值<0.05 被认为具有统计学意义。
2016 年,1204 例(59.9%为男孩,40.1%为女孩)新生儿中,79 例(65.6/1000 例活产儿)死亡。主要入院原因是败血症(35.5%)、呼吸窘迫综合征(15.4%)和围产期窒息(10%)。主要死亡原因是呼吸窘迫综合征(48.1%);极低出生体重(40.9%)和极低出生体重(30.5%)。调整后,低出生体重(调整后的优势比(AOR)=4.55,95%置信区间,1.97-10.50)、极低出生体重(AOR=19.24,95%置信区间,5.80-63.78)、入院时间较晚(诊断后 24 小时内)(AOR=2.96,95%置信区间,1.34-6.52)、阿普加评分(1 分钟时 AOR=2.28,95%置信区间,1.09-4.76,5 分钟时 AOR=2.07,95%置信区间,1.02-4.22)和先天性异常(AOR=3.95,95%置信区间,1.59-9.85)与新生儿死亡率显著相关。在专科新生儿护理病房停留时间>24 小时的新生儿(AOR=0.23,95%置信区间,0.11-0.46)死亡的可能性较低。总体而言,95.8%的新生儿母亲接受了产前护理,96.6%的新生儿在医疗机构分娩。本研究中,母亲的任何情况均与新生儿死亡率无关。
低出生体重、入院时间晚、阿普加评分低和先天性异常与专科新生儿护理病房的新生儿死亡率显著相关。应优先考虑早期管理低出生体重、早产和新生儿并发症,以控制当地新生儿死亡。