Clinical Memory Research Unit, Department of Clinical Sciences, Malmö, Lund University, SE-205 02, Malmö, Sweden.
Memory Clinic, Skåne University Hospital, SE-205 02, Malmö, Sweden.
BMC Neurol. 2020 Jan 9;20(1):10. doi: 10.1186/s12883-019-1591-0.
We investigated the potential associations between cerebro-spinal fluid (CSF) levels of phosphorylated tau (P-tau) and total tau (T-tau) with short-term response to cholinesterase inhibitor (ChEI) treatment, longitudinal outcome and progression rates in Alzheimer's disease (AD).
This prospective, observational study included 129 participants clinically diagnosed with mild-to-moderate AD, who underwent a lumbar puncture. The CSF biomarkers amyloid-β (Aβ), P-tau and T-tau were analysed with xMAP technology. Cognitive, global, instrumental and basic activities of daily living (ADL) capacities at the start of ChEI therapy and semi-annually over 3 years were evaluated.
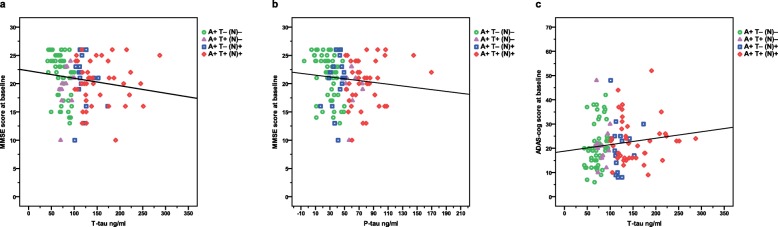
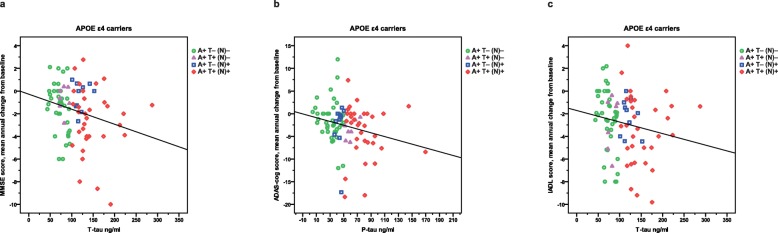
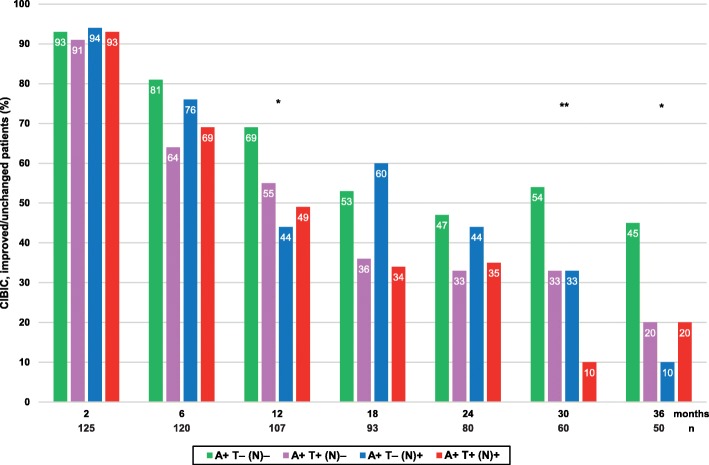
All patients had abnormal Aβ (A+). Fifty-eight individuals (45%) exhibited normal P-tau and T-tau (A+ T- (N)-), 12 (9%) abnormal P-tau/normal T-tau (A+ T+ (N)-), 17 (13%) normal P-tau/abnormal T-tau (A+ T- (N)+) and 42 (33%) abnormal P-tau and T-tau (A+ T+ (N)+). The participants with A+ T+ (N)+ were younger than A+ T- (N)+ at the estimated onset of AD and the initiation of ChEIs. The proportion of 6-month responders to ChEI and deterioration/year after start of treatment did not differ between the AT(N) profiles in any scales. A higher percentage of globally improved/unchanged patients was exhibited in the A+ T- (N)- group after 12, 30 and 36 months of ChEI therapy but not at other assessments. In apolipoprotein E (APOE) ε4-carriers, linear relationships were found between greater cognitive decline/year and higher tau; Mini-Mental State Examination score - T-tau (r = - 0.257, p = 0.014) and Alzheimer's Disease Assessment Scale-cognitive subscale - P-tau (r = - 0.242, p = 0.022). A correlation between faster progression in instrumental ADL (IADL) and higher T-tau was also detected (r = - 0.232, p = 0.028). These associations were not demonstrated in non-ε4-carriers.
Younger age and faster global deterioration were observed in AD patients with pathologic tau and neurodegeneration, whereas more rapid cognitive and IADL decline were related to higher P-tau or T-tau in APOE ε4-carriers only. The results might indicate an association between more pronounced tau pathology/neuronal injury and the APOE ε4-allele leading to a worse prognosis. Our findings showed that the AT(N) biomarker profiles have limited utility to predict AD progression rates and, thus, measure change and interpreting outcomes from clinical trials of future therapies.
我们研究了脑脊液(CSF)中磷酸化 tau(P-tau)和总 tau(T-tau)水平与胆碱酯酶抑制剂(ChEI)治疗的短期反应、阿尔茨海默病(AD)的纵向结局和进展率之间的潜在关联。
这项前瞻性观察性研究纳入了 129 名临床诊断为轻中度 AD 的患者,他们接受了腰椎穿刺。采用 xMAP 技术分析 CSF 生物标志物淀粉样蛋白-β(Aβ)、P-tau 和 T-tau。在 ChEI 治疗开始时和 3 年内每半年评估认知、总体、工具和基本日常生活活动(ADL)能力。
所有患者的 Aβ(A+)均异常。58 名患者(45%)表现为 P-tau 和 T-tau 正常(A+ T- (N)-),12 名患者(9%)表现为 P-tau 异常/ T-tau 正常(A+ T+ (N)-),17 名患者(13%)表现为 P-tau 和 T-tau 均异常(A+ T- (N)+),42 名患者(33%)表现为 P-tau 和 T-tau 均异常(A+ T+ (N)+)。在 AD 发病和 ChEI 开始时,A+ T+ (N)+患者比 A+ T- (N)+患者更年轻。在任何量表中,6 个月时对 ChEI 治疗有反应和治疗开始后恶化/年的比例在 AT(N)特征之间没有差异。在接受 ChEI 治疗 12、30 和 36 个月后,A+ T- (N)-组中全球改善/不变的患者比例更高,但在其他评估中并非如此。在载脂蛋白 E(APOE)ε4 携带者中,发现认知能力下降/年与 tau 水平之间存在线性关系;简易精神状态检查评分-T-tau(r = -0.257,p = 0.014)和阿尔茨海默病评估量表认知子量表-P-tau(r = -0.242,p = 0.022)。还检测到工具性日常生活活动(IADL)进展较快与 T-tau 较高之间存在相关性(r = -0.232,p = 0.028)。在非 ε4 携带者中未发现这些关联。
AD 患者出现病理性 tau 和神经退行性变时,年龄较小,总体恶化较快,而 APOE ε4 携带者中,认知和 IADL 下降较快与 P-tau 或 T-tau 升高有关。结果可能表明 tau 病理学/神经元损伤与 APOE ε4 等位基因之间存在关联,导致预后较差。我们的研究结果表明,AT(N)生物标志物特征对预测 AD 进展率的作用有限,因此,无法衡量未来治疗的临床试验中的变化和解释结果。