Dekker Janneke, Martherus Tessa, Lopriore Enrico, Giera Martin, McGillick Erin V, Hutten Jeroen, van Leuteren Ruud W, van Kaam Anton H, Hooper Stuart B, Te Pas Arjan B
Department of Neonatology, Leiden University Medical Center, Leiden, Netherlands.
Center Proteomics Metabolomics, Leiden University Medical Center, Leiden, Netherlands.
Front Pediatr. 2019 Dec 12;7:504. doi: 10.3389/fped.2019.00504. eCollection 2019.
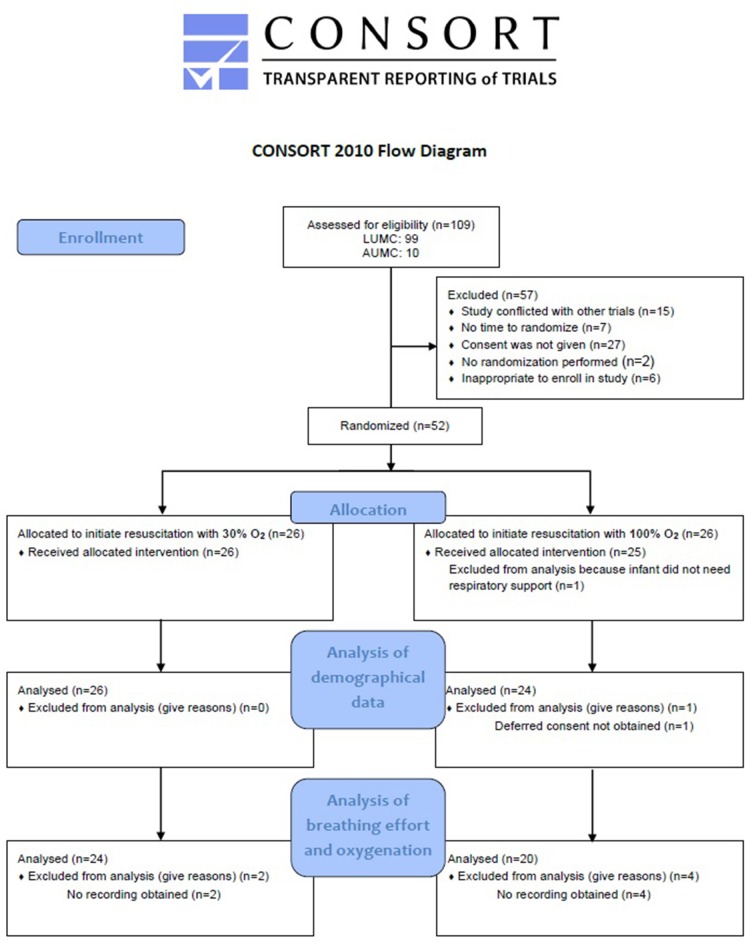
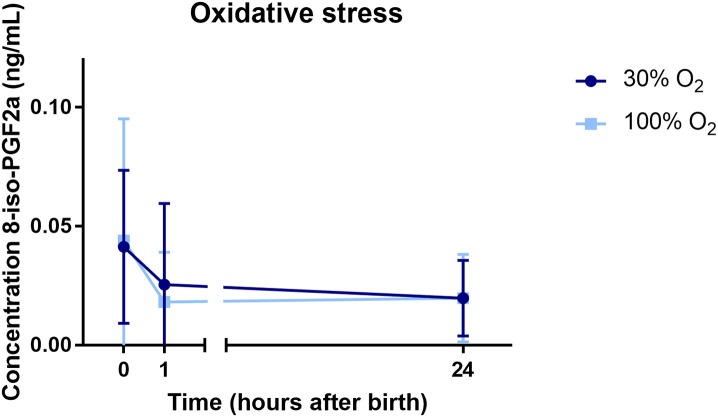
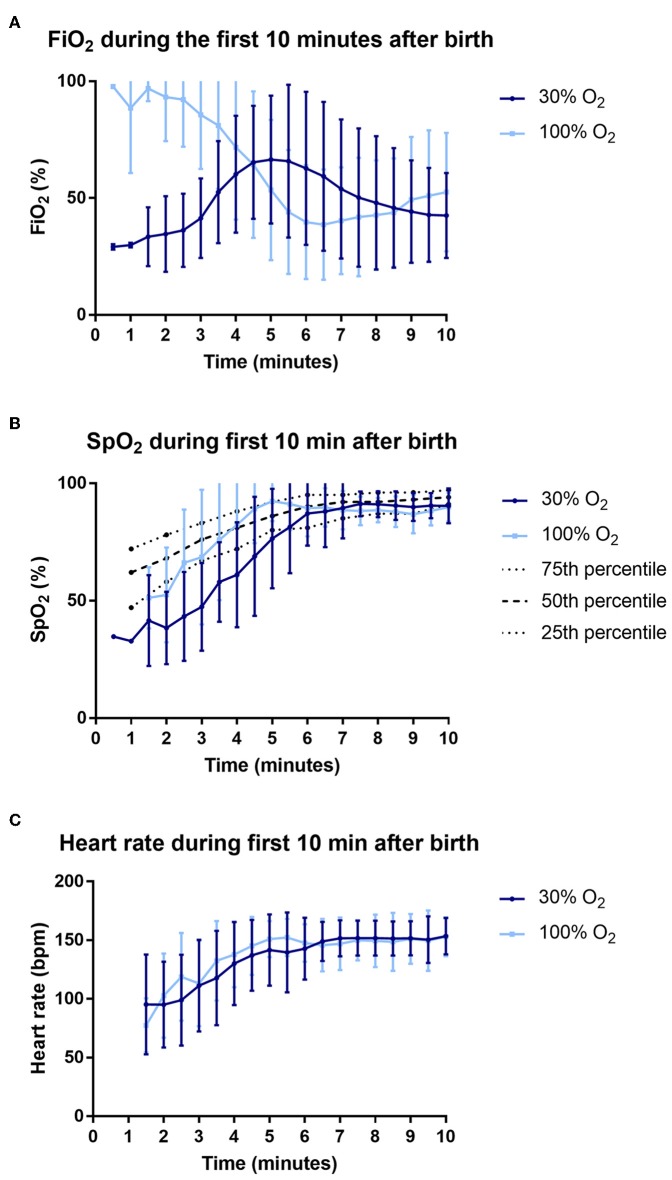
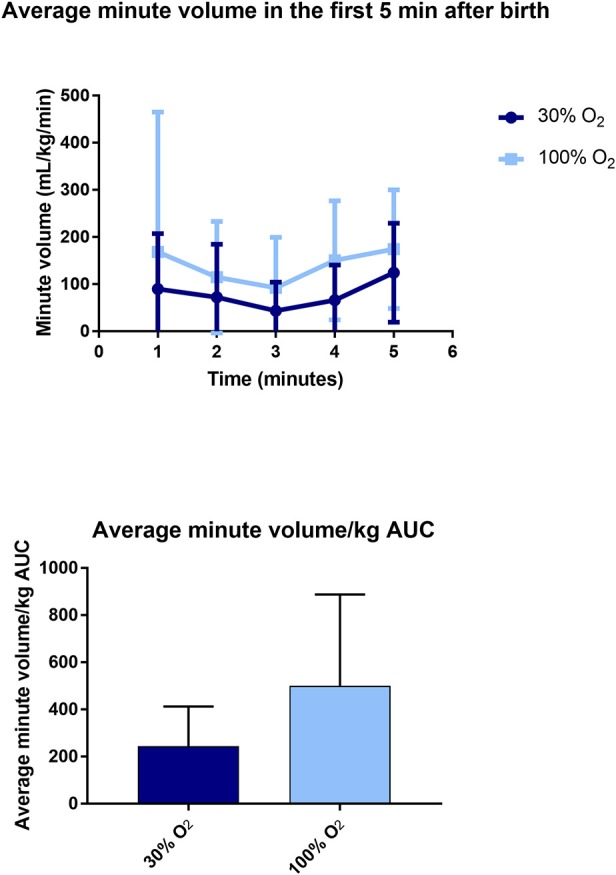
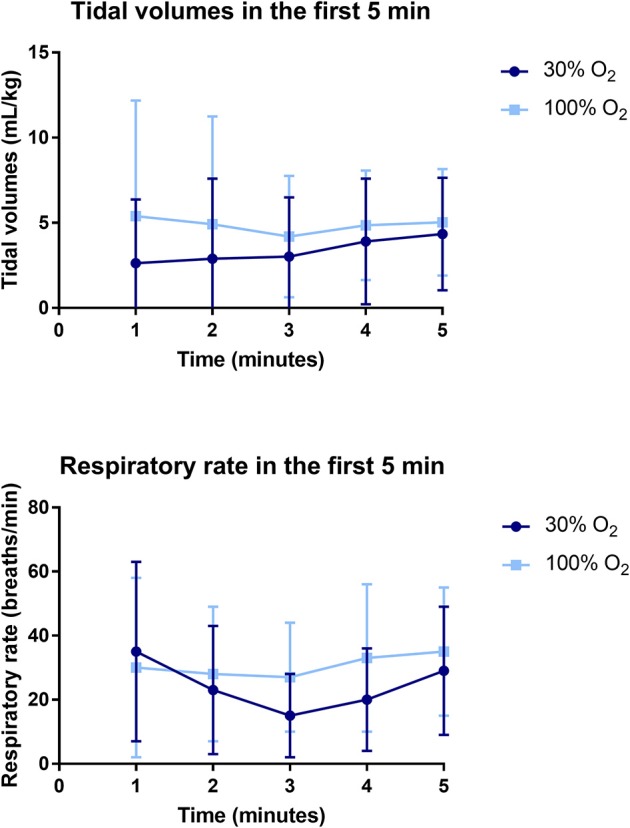
Infants are currently stabilized at birth with initial low FiO which increases the risk of hypoxia and suppression of breathing in the first minutes after birth. We hypothesized that initiating stabilization at birth with a high O concentration, followed by titration, would improve breathing effort when compared to a low O concentration, followed by titration. In a bi-center randomized controlled trial, infants <30 weeks gestation were stabilized at birth with an initial O concentration of 30 or 100%, followed by oxygen titration. Primary outcome was minute volume of spontaneous breathing. We also assessed tidal volumes, mean inspiratory flow rate (MIFR) and respiratory rate with a respiratory function monitor in the first 5 min after birth, and evaluated the duration of mask ventilation in the first 10 min after birth. Pulse oximetry was used to measure heart rate and SpO values in the first 10 min. Hypoxemia was defined as SpO < 25th percentile and hyperoxemia as SpO >95%. 8-iso-prostaglandin F2α (8iPGF2α) was measured to assess oxidative stress in cord blood and 1 and 24 h after birth. Fifty-two infants were randomized and recordings were obtained in 44 infants (100% O-group: = 20, 30% O-group: = 24). Minute volumes were significantly higher in the 100% O-group (146.34 ± 112.68 mL/kg/min) compared to the 30% O-group (74.43 ± 52.19 mL/kg/min), = 0.014. Tidal volumes and MIFR were significantly higher in the 100% O-group, while the duration of mask ventilation given was significantly shorter. Oxygenation in the first 5 min after birth was significantly higher in infants in the 100% O-group [85 (64-93)%] compared to the 30% O-group [58 (46-67)%], < 0.001. The duration of hypoxemia was significantly shorter in the 100% O-group, while the duration of hyperoxemia was not different between groups. There was no difference in oxidative stress marker 8iPGF2α between the groups. Initiating stabilization of preterm infants at birth with 100% O led to higher breathing effort, improved oxygenation, and a shorter duration of mask ventilation as compared to 30% O, without increasing the risk for hyperoxia or oxidative stress. This study was registered in www.trialregister.nl, with registration number NTR6878.
目前,婴儿出生时通过初始低氧浓度进行稳定处理,这增加了出生后最初几分钟内缺氧和呼吸抑制的风险。我们假设,与低氧浓度起始并随后进行滴定相比,以高氧浓度起始出生时的稳定处理并随后进行滴定,将改善呼吸努力。在一项双中心随机对照试验中,孕周小于30周的婴儿出生时以30%或100%的初始氧浓度进行稳定处理,随后进行氧滴定。主要结局是自主呼吸分钟通气量。我们还在出生后前5分钟使用呼吸功能监测仪评估潮气量、平均吸气流量率(MIFR)和呼吸频率,并评估出生后前10分钟面罩通气的持续时间。在出生后前10分钟使用脉搏血氧饱和度仪测量心率和SpO₂值。低氧血症定义为SpO₂<第25百分位数,高氧血症定义为SpO₂>95%。测量8-异前列腺素F2α(8iPGF2α)以评估脐带血以及出生后1小时和24小时的氧化应激。52名婴儿被随机分组,44名婴儿获得了记录(100%氧组:n = 20,30%氧组:n = 24)。100%氧组的分钟通气量(146.34±112.68 mL/kg/min)显著高于30%氧组(74.43±52.19 mL/kg/min),P = 0.014。100%氧组的潮气量和MIFR显著更高,而给予的面罩通气持续时间显著更短。出生后前5分钟,100%氧组婴儿的氧合(85[64 - 93]%)显著高于30%氧组[58(46 - 67)%],P < 0.001。100%氧组的低氧血症持续时间显著更短,而两组间高氧血症持续时间无差异。两组间氧化应激标志物8iPGF2α无差异。与30%氧相比,出生时以100%氧起始对早产儿进行稳定处理可导致更高的呼吸努力、改善氧合以及更短的面罩通气持续时间,且不增加高氧或氧化应激风险。本研究已在www.trialregister.nl注册,注册号为NTR6878。