Department of Community Health and Epidemiology, Health Sciences Building, 107 Wiggins Road, Saskatoon, SK, S7N 5E5, Canada.
Department of Psychology, University of Saskatchewan Arts, 154, 9 Campus Drive, Saskatoon, SK, S7N 5A5, Canada.
BMC Health Serv Res. 2020 Jan 23;20(1):59. doi: 10.1186/s12913-019-4649-1.
Shared Decision-making (SDM), a medical decision-making model, was popularized in the late 1980s in reaction to then predominate paternalistic decision-making, aiming to better meet the needs of patients. Extensive research has been conducted internationally examining the benefits of SDM implementation; however, existing theory on how SDM works, for whom, in which circumstances, and why is limited. While literature has shown positive patient, health care provider, and system benefits (SDM outputs), further research is required to understand the nuances of this type of decision-making. As such, we set out to address: "In which situations, how, why, and for whom does SDM between patients and health care providers contribute to improved engagement in the Shared Decision-making process?"
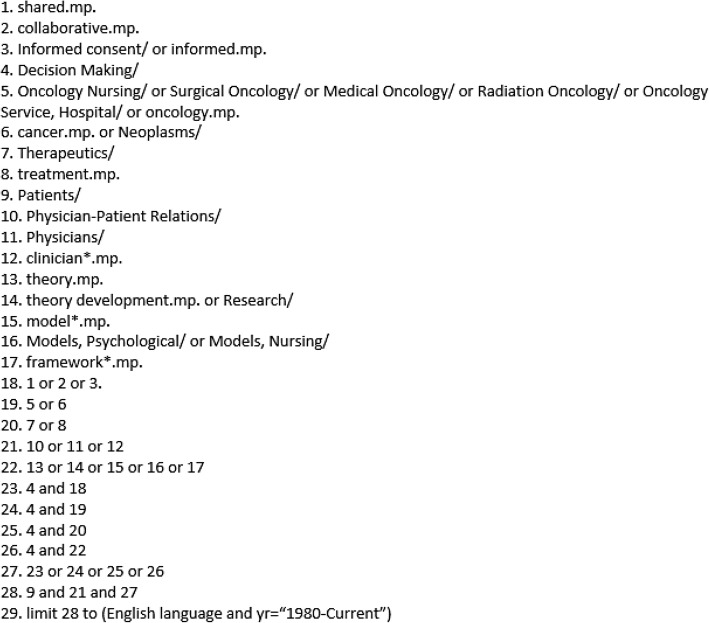
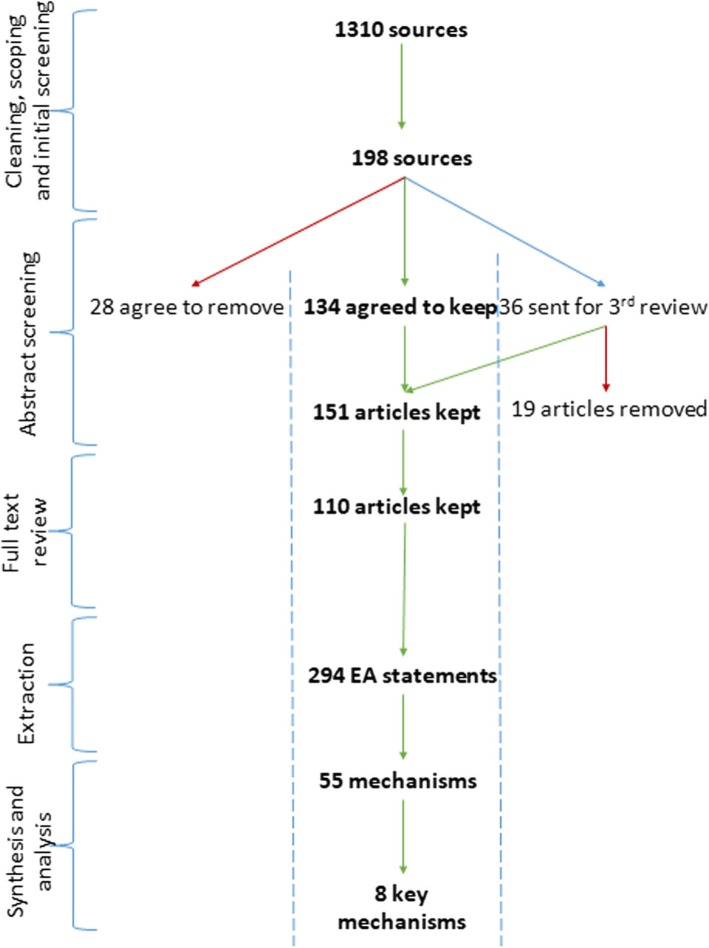
To achieve our study goals we conducted a seven-step realist synthesis process, which included: (1) preliminary program theory development, (2) search strategy development, (3) selection and appraisal of literature in accordance with realist methodology, (4) data extraction, (5) identification of relevant formal theories, (6) data analysis and synthesis, and (7) formation of a revised program theory with the input of stakeholders. This process was done in accordance with RAMESES guidelines and publication standards for a realist synthesis. Expert consultations were also held to ensure consistency within the SDM literature.
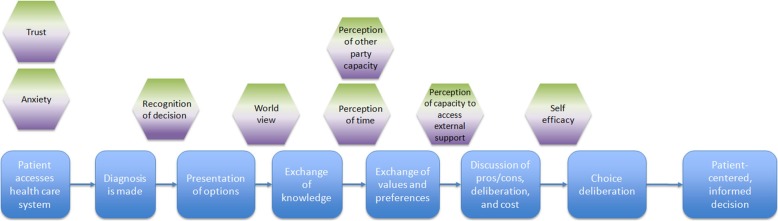
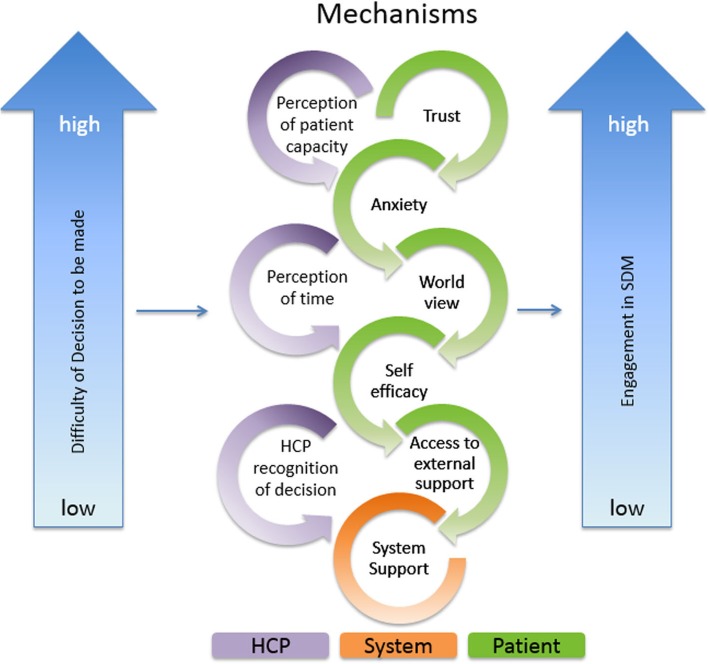
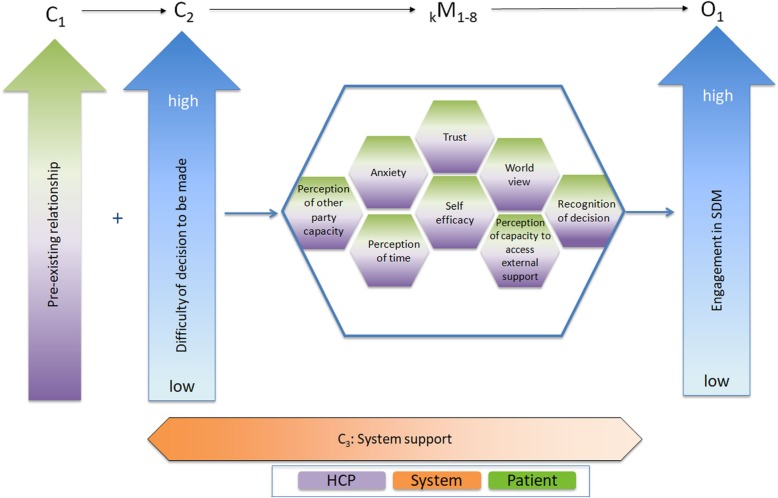
Through our realist synthesis, we developed a program theory of SDM which includes three contexts (pre-existing relationship, difficulty of decision, and system support), eight mechanism sets (anxiety, trust, perception of other party capacity, perception of time, self-efficacy, world view, perception of capacity to external support, and recognition of decision), and one outcome (engagement in SDM).
As far as the authors of this paper are aware, this paper is the first to begin unpacking how SDM works, for whom, in which circumstances, and why. By examining key mechanism sets and exploring how they facilitate or inhibit SDM, we have produced a program theory that may assist health care professionals, policy makers, and patients. While further research is suggested to further unpack the concepts identified within this paper, this provides an initial understanding into the theory behind SDM.
PROSPERO: CRD42017062609.
共享决策(SDM)是一种医学决策模型,于 20 世纪 80 年代末在主导的家长式决策模式基础上发展而来,旨在更好地满足患者的需求。国际上已经开展了广泛的研究,以检验 SDM 实施的益处;然而,关于 SDM 如何运作、为谁、在何种情况下以及为何运作的现有理论是有限的。虽然文献表明 SDM 对患者、医疗保健提供者和系统有积极的影响(SDM 输出),但需要进一步研究以了解这种决策类型的细微差别。因此,我们着手解决以下问题:“在哪些情况下,患者和医疗保健提供者之间的 SDM 如何、为何以及为谁有助于改善共享决策过程的参与度?”
为了实现我们的研究目标,我们进行了七步的现实主义综合过程,包括:(1)初步方案理论发展;(2)根据现实主义方法论制定搜索策略;(3)按照方案理论选择和评估文献;(4)数据提取;(5)识别相关的正式理论;(6)数据分析和综合;(7)在利益相关者的参与下形成修订后的方案理论。该过程符合 RAMESES 指南和现实主义综合的出版标准。还举行了专家咨询会议,以确保 SDM 文献的一致性。
通过我们的现实主义综合,我们开发了一个 SDM 的方案理论,包括三个背景(预先存在的关系、决策的难度和系统支持)、八个机制集(焦虑、信任、对对方能力的感知、对时间的感知、自我效能、世界观、对外部支持能力的感知和对决策的认知)和一个结果(参与 SDM)。
据本文作者所知,这篇论文是第一份开始剖析 SDM 如何运作、为谁、在何种情况下以及为何运作的论文。通过检查关键的机制集,并探索它们如何促进或抑制 SDM,我们提出了一个可能有助于医疗保健专业人员、政策制定者和患者的方案理论。虽然建议进一步研究以进一步剖析本文中确定的概念,但这为 SDM 的理论提供了初步理解。
PROSPERO:CRD42017062609。