Minen Mia T, Sahyoun Gabriella, Gopal Ariana, Levitan Valeriya, Pirraglia Elizabeth, Simon Naomi M, Halpern Audrey
Department of Neurology, New York University Langone Health, New York, NY, USA.
Department of Neuroscience, Barnard College, Columbia University, New York, NY, USA.
Headache. 2020 Feb;60(2):441-456. doi: 10.1111/head.13738. Epub 2020 Jan 24.
Relaxation, biofeedback, and cognitive behavioral therapy are evidence-based behavioral therapies for migraine. Despite such efficacy, research shows that only about half of patients initiate behavioral therapy recommended by their headache specialists.
Motivational interviewing (MI) is a widely used method to help patients explore and overcome ambivalence to enact positive life changes. We tested the hypothesis that telephone-based MI would improve initiation, scheduling, and attending behavioral therapy for migraine.
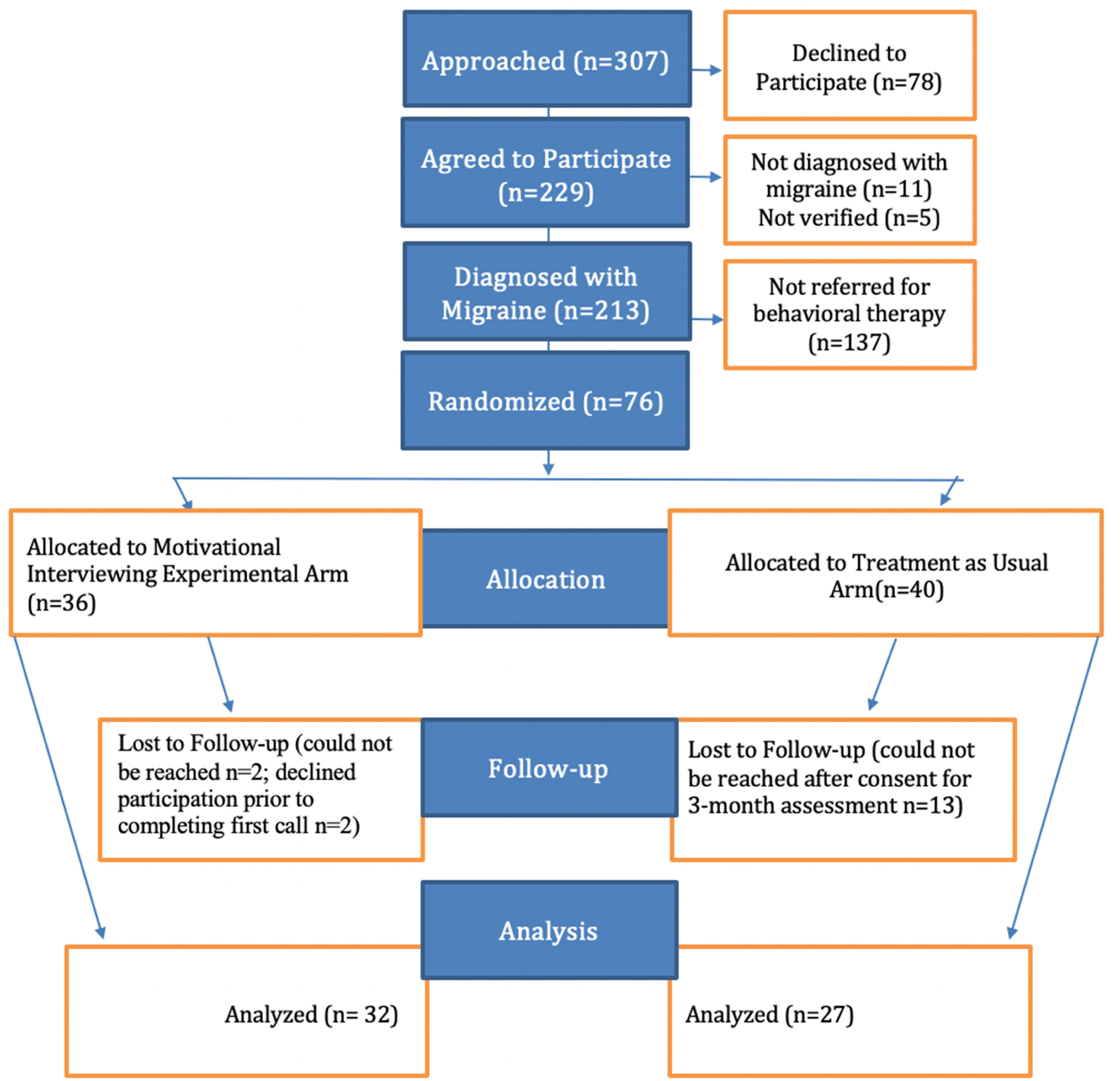
Single-blind randomized controlled trial comparing telephone-based MI to treatment as usual (TAU). Participants were recruited during their appointments with headache specialists at two sites of a New York City medical center.
ages from 16 to 80, migraine diagnosis by United Council of Neurologic Subspecialty fellowship trained and/or certified headache specialist, and referral for behavioral therapy for prevention in the appointment of recruitment.
having done behavioral therapy for migraine in the past year. Participants in the MI group received up to 5 MI calls. TAU participants were called after 3 months for general follow-up data. The prespecified primary outcome was scheduling a behavioral therapy appointment, and secondary outcomes were initiating and attending a behavioral therapy appointment.
76 patients were enrolled and randomized (MI = 36, TAU = 40). At baseline, the mean number of headache days was 12.0 ± 9.0. Self-reported anxiety was present for 36/52 (69.2%) and depression for 30/52 (57.7%). Follow-up assessments were completed for 77.6% (59/76, MI = 32, TAU = 27). The mean number of MI calls per participant was 2.69 ± 1.56 [0 to 5]. There was a greater likelihood of those in the MI group to initiating an appointment (22/32, 68.8% vs 11/27, 40.7%, P = .0309). There were no differences in appointment scheduling or attendance. Reasons stated for not initiating behavioral therapy were lack of time, lack of insurance/funding, prioritizing other treatments, and travel plans.
Brief telephone-based MI may improve rates of initiation of behavioral therapy for migraine, but other barriers appear to lessen the impact on scheduling and attending behavioral therapy appointments.
放松疗法、生物反馈疗法和认知行为疗法是基于证据的偏头痛行为疗法。尽管有如此疗效,但研究表明,只有约一半的患者开始接受头痛专科医生推荐的行为疗法。
动机性访谈(MI)是一种广泛使用的方法,可帮助患者探索并克服矛盾心理,以实现积极的生活改变。我们检验了以下假设:基于电话的动机性访谈能改善偏头痛行为疗法的启动、安排和参与情况。
单盲随机对照试验,将基于电话的动机性访谈与常规治疗(TAU)进行比较。参与者是在纽约市一家医疗中心的两个地点与头痛专科医生预约就诊时招募的。
年龄在16至80岁之间,由美国神经科专科联合委员会奖学金培训和/或认证的头痛专科医生诊断为偏头痛,且在招募预约时被转诊接受预防行为疗法。
在过去一年中接受过偏头痛行为疗法。MI组的参与者最多接受5次MI电话访谈。TAU组的参与者在3个月后被电话随访以获取一般随访数据。预先设定的主要结局是安排行为疗法预约,次要结局是开始并参加行为疗法预约。
76名患者被纳入并随机分组(MI组 = 36人,TAU组 = 40人)。基线时,平均头痛天数为12.0 ± 9.0天。自我报告有焦虑症状的有36/52(69.2%),有抑郁症状的有30/52(57.7%)。77.6%(59/76)的患者完成了随访评估(MI组 = 32人,TAU组 = 27人)。每位参与者平均接受的MI电话访谈次数为2.69 ± 1.56次[0至5次]。MI组的患者更有可能开始预约(22/32,68.8%对11/27,40.7%,P = 0.0309)。在预约安排或就诊方面没有差异。未开始行为疗法的原因包括时间不足、缺乏保险/资金、优先考虑其他治疗以及旅行计划。
简短的基于电话的动机性访谈可能会提高偏头痛行为疗法的启动率,但其他障碍似乎会减弱其对行为疗法预约安排和就诊的影响。