Michelle L. Sloan, MA, and Michael J. Park, PhD, are Health Scientists, Division of Global Health Protection, Center for Global Health, Centers for Disease Control and Prevention, Atlanta, GA. Brigette L. Gleason, MD, is Surveillance and Program Lead, and Fanny F. Koroma, MSc, is a Public Health Surveillance Specialist; both at the CDC Sierra Leone Country Office, Division of Global Health Protection, Center for Global Health, Centers for Disease Control and Prevention, Freetown, Sierra Leone. James S. Squire, MIPH, is Program Manager, and Solomon Aiah Sogbeh is Senior Public Health Superintendent; both at the National Disease Surveillance Program, Ministry of Health and Sanitation, Freetown, Sierra Leone. The views expressed are the authors' own and do not necessarily represent the views of the Ministry of Health and Sanitation or the US Centers for Disease Control and Prevention.
Health Secur. 2020 Jan;18(S1):S64-S71. doi: 10.1089/hs.2019.0082.
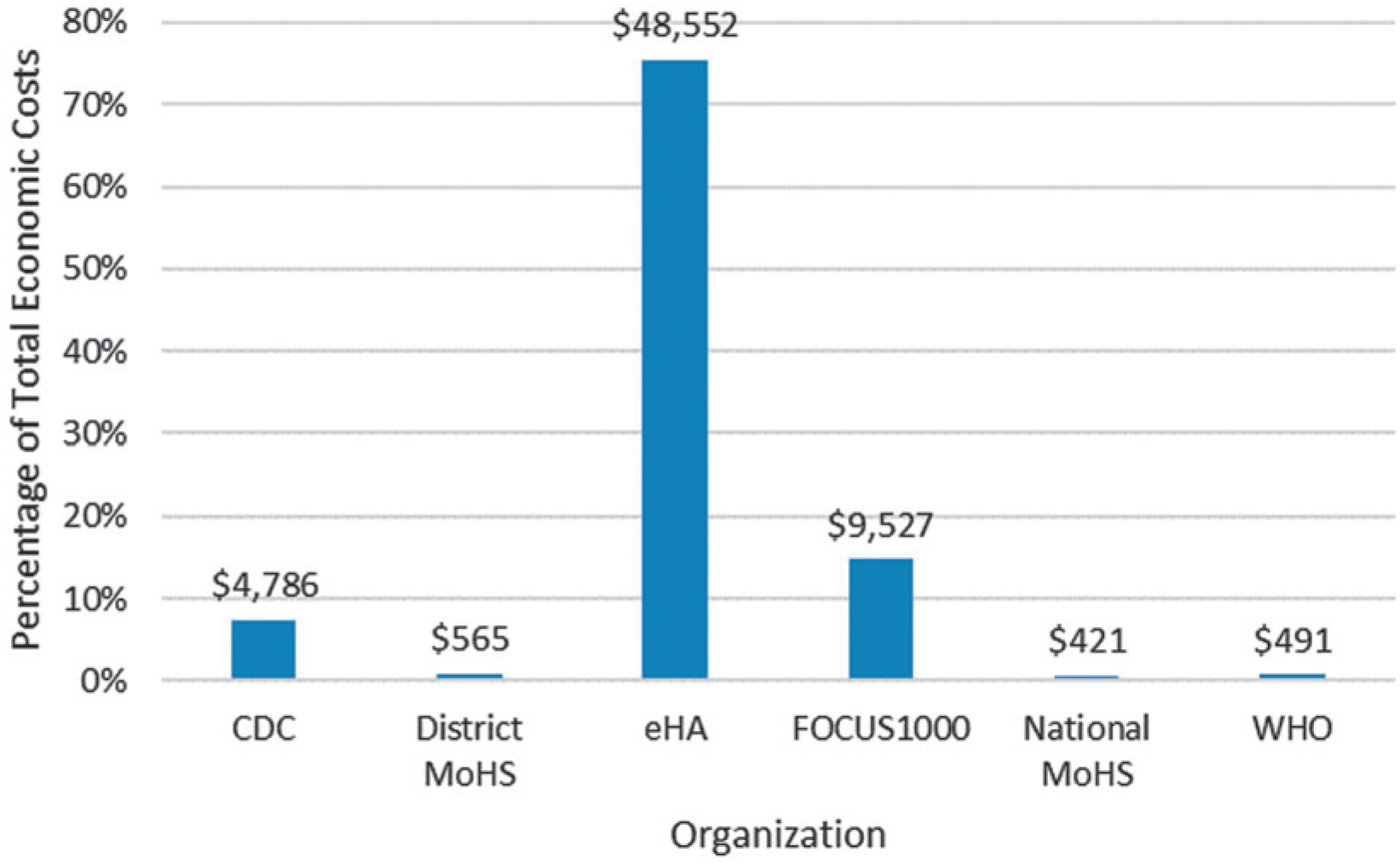
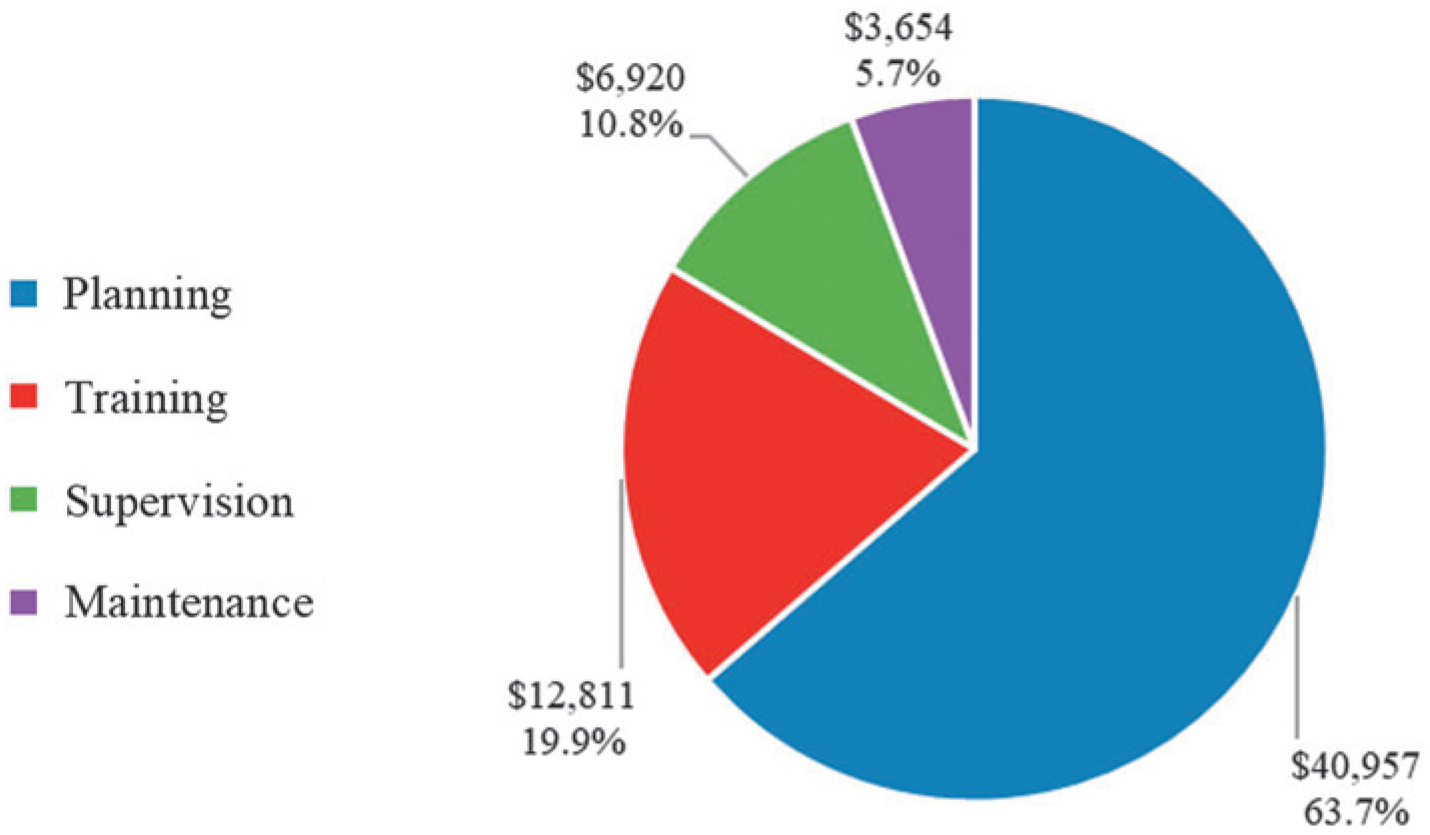
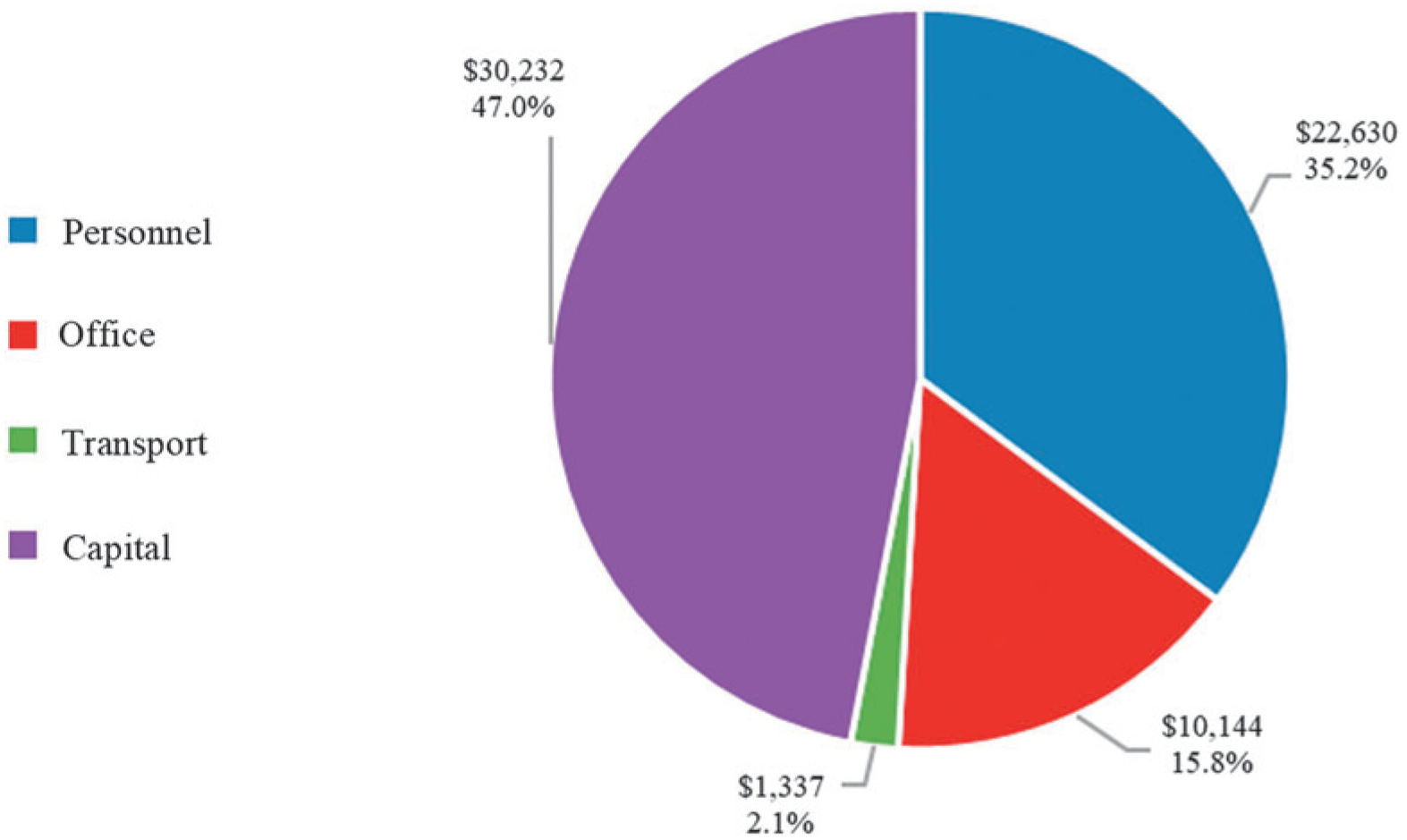
Global health security depends on effective surveillance systems to prevent, detect, and respond to disease threats. Real-time surveillance initiatives aim to develop electronic systems to improve reporting and analysis of disease data. Sierra Leone, with the support of Global Health Security Agenda partners, developed an electronic Integrated Disease Surveillance and Response (eIDSR) system capable of mobile reporting from health facilities. We estimated the economic costs associated with rollout of health facility eIDSR in the Western Area Rural district in Sierra Leone and projected annual direct operational costs. Cost scenarios with increased transport costs, decreased use of partner personnel, and altered cellular data costs were modeled. Cost data associated with activities were retrospectively collected and were assessed across rollout phases. Costs were organized into cost categories: personnel, office operating, transport, and capital. We estimated costs by category and phase and calculated per health facility and per capita costs. The total economic cost to roll out eIDSR to the Western Area Rural district over the 14-week period was US$64,342, a per health facility cost of $1,021. Equipment for eIDSR was the primary cost driver (45.5%), followed by personnel (35.2%). Direct rollout costs were $38,059, or 59.2% of total economic costs. The projected annual direct operational costs were $14,091, or $224 per health facility. Although eIDSR equipment costs are a large portion of total costs, annual direct operational costs are projected to be minimal once the system is implemented. Our findings can be used to make decisions about establishing and maintaining electronic, real-time surveillance in Sierra Leone and other low-resource settings.
全球卫生安全依赖于有效的监测系统,以预防、发现和应对疾病威胁。实时监测计划旨在开发电子系统,以改进疾病数据的报告和分析。在全球卫生安全议程合作伙伴的支持下,塞拉利昂开发了一个能够从卫生机构进行移动报告的电子综合疾病监测和应对 (eIDSR) 系统。我们估计了在塞拉利昂西部农村地区推出卫生机构 eIDSR 的相关经济成本,并预测了每年的直接运营成本。我们对增加运输成本、减少合作伙伴人员使用以及改变蜂窝数据成本的成本情景进行了建模。与活动相关的成本数据是回顾性收集的,并在推出阶段进行了评估。成本分为人员、办公运营、运输和资本四类。我们按类别和阶段估算了成本,并计算了每个卫生机构和每人的成本。在 14 周的时间内,在西部农村地区推出 eIDSR 的总经济成本为 64342 美元,每个卫生机构的成本为 1021 美元。eIDSR 设备是主要成本驱动因素(45.5%),其次是人员(35.2%)。直接推出成本为 38059 美元,占总经济成本的 59.2%。预计每年的直接运营成本为 14091 美元,即每个卫生机构 224 美元。尽管 eIDSR 设备成本是总成本的很大一部分,但一旦系统实施,预计每年的直接运营成本将非常低。我们的研究结果可用于在塞拉利昂和其他资源匮乏的环境中做出关于建立和维护电子实时监测的决策。