Lokuge Kamalini, Caleo Grazia, Greig Jane, Duncombe Jennifer, McWilliam Nicholas, Squire James, Lamin Manjo, Veltus Emily, Wolz Anja, Kobinger Gary, de la Vega Marc-Antoine, Gbabai Osman, Nabieu Sao, Lamin Mohammed, Kremer Ronald, Danis Kostas, Banks Emily, Glass Kathryn
Manson Unit, Médecins Sans Frontières, London, United Kingdom.
National Centre for Epidemiology and Population Health, Research School of Population Health, Australian National University, Canberra, Australia.
PLoS Negl Trop Dis. 2016 Mar 9;10(3):e0004498. doi: 10.1371/journal.pntd.0004498. eCollection 2016 Mar.
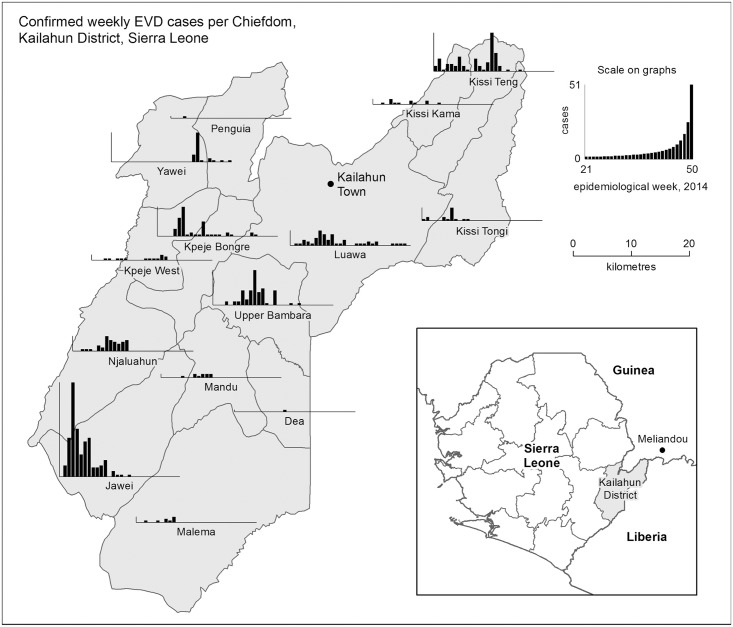
The scale and geographical distribution of the current outbreak in West Africa raised doubts as to the effectiveness of established methods of control. Ebola Virus Disease (EVD) was first detected in Sierra Leone in May 2014 in Kailahun district. Despite high case numbers elsewhere in the country, transmission was eliminated in the district by December 2014. We describe interventions underpinning successful EVD control in Kailahun and implications for EVD control in other areas.
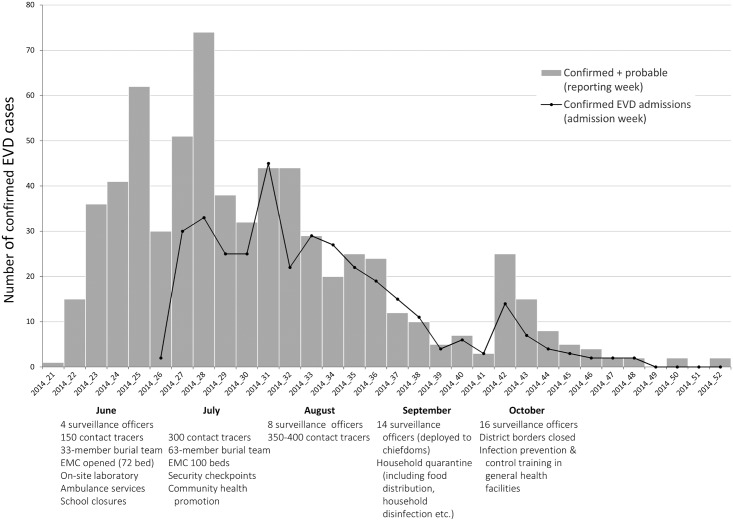
Internal service data and published reports from response agencies were analysed to describe the structure and type of response activities, EVD case numbers and epidemic characteristics. This included daily national situation reports and District-level data and reports of the Sierra Leone Ministry of Health and Sanitation, and Médecins Sans Frontières (MSF) patient data and internal epidemiological reports. We used EVD case definitions provided by the World Health Organisation over the course of the outbreak. Characteristics assessed included level of response activities and epidemiological features such as reported exposure (funeral-related or not), time interval between onset of illness and admission to the EVD Management Centre (EMC), work-related exposures (health worker or not) and mortality. We compared these characteristics between two time periods--June to July (the early period of response), and August to December (when coverage and quality of response had improved). A stochastic model was used to predict case numbers per generation with different numbers of beds and a varying percentage of community cases detected.
There were 652 probable/confirmed EVD cases from June-December 2014 in Kailahun. An EMC providing patient care opened in June. By August 2014 an integrated detection, treatment, and prevention strategy was in place across the district catchment zone. From June-July to August-December 2014 surveillance and contact tracing staff increased from 1.0 to 8.8 per confirmed EVD case, EMC capacity increased from 32 to 100 beds, the number of burial teams doubled, and health promotion activities increased in coverage. These improvements in response were associated with the following changes between the same periods: the proportion of confirmed/probable cases admitted to the EMC increased from 35% to 83% (χ(2) p-value<0·001), the proportion of confirmed patients admitted to the EMC <3 days of symptom onset increased from 19% to 37% (χ(2) p-value <0·001), and reported funeral contact in those admitted decreased from 33% to 16% (χ(2) p-value <0·001). Mathematical modelling confirmed the importance of both patient management capacity and surveillance and contact tracing for EVD control.
Our findings demonstrate that control of EVD can be achieved using established interventions based on identification and appropriate management of those who are at risk of and develop EVD, including in the context of ongoing transmission in surrounding regions. Key attributes in achieving control were sufficient patient care capacity (including admission to specialist facilities of suspect and probable cases for assessment), integrated with adequate staffing and resourcing of community-based case detection and prevention activities. The response structure and coverage targets we present are of value in informing effective control in current and future EVD outbreaks.
当前西非疫情的规模和地理分布引发了人们对既定防控方法有效性的质疑。2014年5月,在凯拉洪区首次在塞拉利昂检测到埃博拉病毒病(EVD)。尽管该国其他地区病例数众多,但到2014年12月,该地区的传播已被消除。我们描述了凯拉洪成功控制埃博拉病毒病的干预措施及其对其他地区埃博拉病毒病防控的启示。
分析内部服务数据和应对机构发布的报告,以描述应对活动的结构和类型、埃博拉病毒病病例数及疫情特征。这包括每日国家情况报告、塞拉利昂卫生与环境部的地区级数据和报告,以及无国界医生组织(MSF)的患者数据和内部流行病学报告。我们采用了世界卫生组织在疫情期间提供的埃博拉病毒病病例定义。评估的特征包括应对活动水平和流行病学特征,如报告的暴露情况(与葬礼相关或无关)、发病至入住埃博拉病毒病管理中心(EMC)的时间间隔、与工作相关的暴露情况(是否为卫生工作者)以及死亡率。我们比较了两个时间段——6月至7月(应对初期)和8月至12月(应对覆盖范围和质量有所改善时)的这些特征。使用随机模型预测不同病床数量和不同比例社区病例被检测到时每一代的病例数。
2014年6月至12月,凯拉洪有652例疑似/确诊埃博拉病毒病病例。6月开设了一家提供患者护理的埃博拉病毒病管理中心。到2014年8月,整个地区集水区实施了综合检测、治疗和预防策略。从2014年6月至7月到8月至12月,每例确诊埃博拉病毒病病例的监测和接触者追踪工作人员从1.0人增加到8.8人,埃博拉病毒病管理中心的床位从32张增加到100张,埋葬小组数量翻倍,健康促进活动的覆盖范围扩大。应对措施的这些改进与同期的以下变化相关:入住埃博拉病毒病管理中心的确诊/疑似病例比例从35%增加到83%(χ(2) p值<0.001),症状出现后<3天入住埃博拉病毒病管理中心的确诊患者比例从19%增加到37%(χ(2) p值<0.001),入住者中报告的葬礼接触比例从33%降至16%(χ(2) p值<0.001)。数学模型证实了患者管理能力以及监测和接触者追踪对埃博拉病毒病防控的重要性。
我们的研究结果表明,基于识别和适当管理有埃博拉病毒病风险及已感染埃博拉病毒病的人群,利用既定干预措施可以实现对埃博拉病毒病的控制,包括在周边地区仍有传播的情况下。实现控制的关键因素是足够的患者护理能力(包括将疑似和可能病例收治到专科设施进行评估),并与基于社区的病例检测和预防活动的充足人员配备和资源配置相结合。我们提出的应对结构和覆盖目标对于指导当前和未来埃博拉病毒病疫情的有效控制具有价值。