South African Medical Research Council Centre for Tuberculosis Research, DST NRF Centre of Excellence for Biomedical Tuberculosis research, Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
Global Health Institute, Epidemiology and Social Medicine, University of Antwerp, Antwerp, Belgium.
BMC Med. 2020 Feb 4;18(1):24. doi: 10.1186/s12916-019-1487-2.
Atypical Beijing genotype Mycobacterium tuberculosis strains are widespread in South Africa and have acquired resistance to up to 13 drugs on multiple occasions. It is puzzling that these strains have retained fitness and transmissibility despite the potential fitness cost associated with drug resistance mutations.
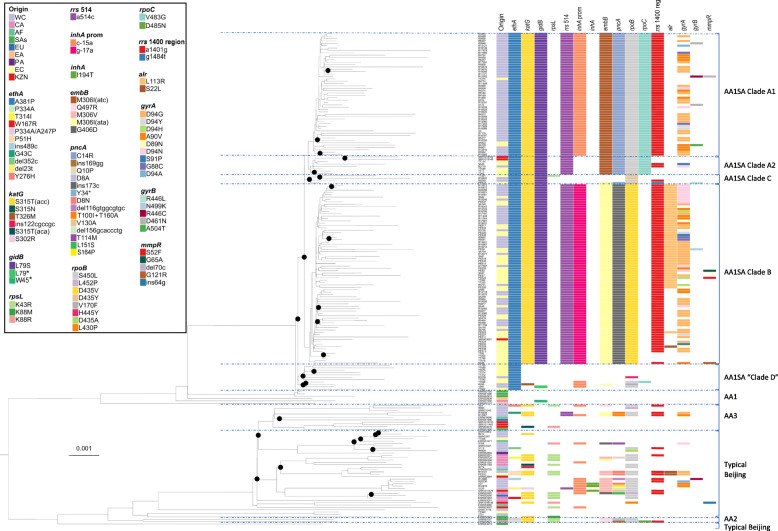
We conducted Illumina sequencing of 211 Beijing genotype M. tuberculosis isolates to facilitate the detection of genomic features that may promote acquisition of drug resistance and restore fitness in highly resistant atypical Beijing forms. Phylogenetic and comparative genomic analysis was done to determine changes that are unique to the resistant strains that also transmit well. Minimum inhibitory concentration (MIC) determination for streptomycin and bedaquiline was done for a limited number of isolates to demonstrate a difference in MIC between isolates with and without certain variants.
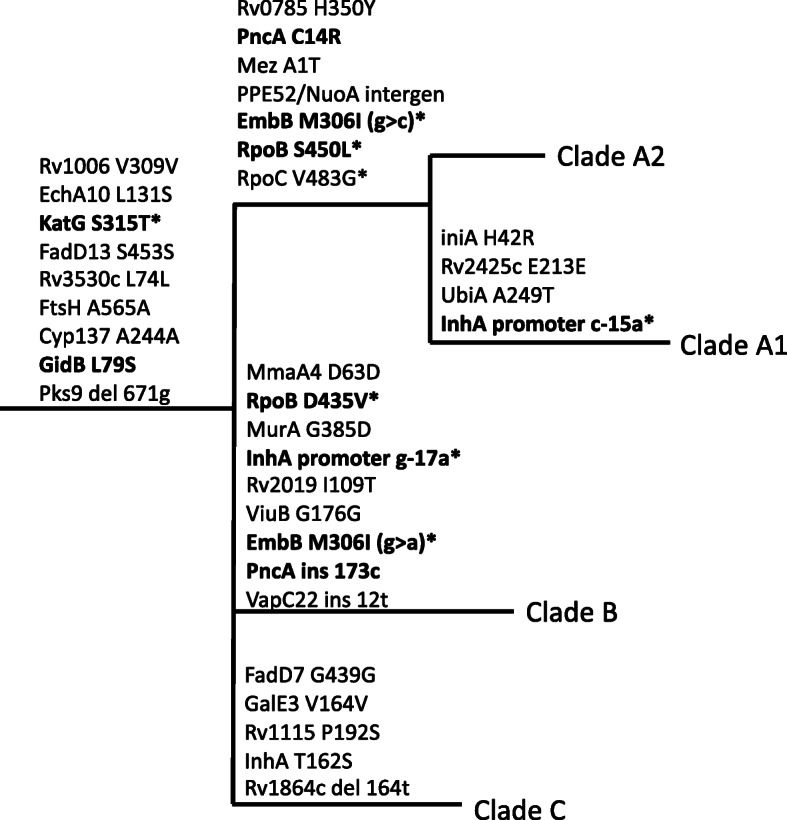
Phylogenetic analysis confirmed that two clades of atypical Beijing strains have independently developed resistance to virtually all the potent drugs included in standard (pre-bedaquiline) drug-resistant TB treatment regimens. We show that undetected drug resistance in a progenitor strain was likely instrumental in this resistance acquisition. In this cohort, ethionamide (ethA A381P) resistance would be missed in first-line drug-susceptible isolates, and streptomycin (gidB L79S) resistance may be missed due to an MIC close to the critical concentration. Subsequent inadequate treatment historically led to amplification of resistance and facilitated spread of the strains. Bedaquiline resistance was found in a small number of isolates, despite lack of exposure to the drug. The highly resistant clades also carry inhA promoter mutations, which arose after ethA and katG mutations. In these isolates, inhA promoter mutations do not alter drug resistance, suggesting a possible alternative role.
The presence of the ethA mutation in otherwise susceptible isolates from ethionamide-naïve patients demonstrates that known exposure is not an adequate indicator of drug susceptibility. Similarly, it is demonstrated that bedaquiline resistance can occur without exposure to the drug. Inappropriate treatment regimens, due to missed resistance, leads to amplification of resistance, and transmission. We put these results into the context of current WHO treatment regimens, underscoring the risks of treatment without knowledge of the full drug resistance profile.
非典型北京基因型结核分枝杆菌菌株广泛存在于南非,并多次获得对多达 13 种药物的耐药性。令人困惑的是,尽管耐药突变与潜在的适应度成本相关,但这些菌株仍然保持着适应性和传染性。
我们对 211 株北京基因型结核分枝杆菌进行了 Illumina 测序,以促进检测可能促进耐药性获得并恢复高度耐药非典型北京形式适应性的基因组特征。进行了系统发育和比较基因组分析,以确定仅存在于耐药菌株中且传播良好的菌株的特有变化。对少数分离株进行了链霉素和贝达喹啉的最低抑菌浓度 (MIC) 测定,以证明具有某些变体的分离株与不具有某些变体的分离株之间的 MIC 存在差异。
系统发育分析证实,两个非典型北京菌株的分枝已独立地对标准(贝达喹啉前)耐药结核病治疗方案中包含的几乎所有强效药物产生耐药性。我们表明,祖代菌株中未检测到的耐药性可能是这种耐药性获得的关键。在该队列中,由于 MIC 接近临界浓度,利福平(ethA A381P)耐药性可能在一线药物敏感分离株中被遗漏,而链霉素(gidB L79S)耐药性可能因 MIC 而被遗漏。由于治疗不足,历史上导致耐药性扩增并促进了菌株的传播。尽管未暴露于该药物,但在少数分离株中发现了贝达喹啉耐药性。高度耐药的分枝也携带 inhA 启动子突变,该突变在 ethA 和 katG 突变之后出现。在这些分离株中,inhA 启动子突变不改变药物耐药性,这表明可能存在替代作用。
在来自未曾使用过乙硫异烟胺的患者的、对乙硫异烟胺敏感的分离株中存在 ethA 突变表明,已知的暴露并不能充分表明药物敏感性。同样,没有暴露于药物也可以发生贝达喹啉耐药性。由于耐药性漏检导致不适当的治疗方案会导致耐药性扩增和传播。我们将这些结果置于当前世界卫生组织治疗方案的背景下,强调了在不了解完整药物耐药谱的情况下进行治疗的风险。