Department of Eye and Vision, University of Liverpool, Liverpool, UK.
Respiratory Medicine, Sir Charles Gairdner Hospital, Perth, Australia.
BMC Med Res Methodol. 2020 Feb 5;20(1):22. doi: 10.1186/s12874-020-0913-7.
Clinical prediction models are widely used to guide medical advice and therapeutic interventions. Asthma is one of the most common chronic diseases globally and is characterised by acute deteriorations. These exacerbations are largely preventable, so there is interest in using clinical prediction models in this area. The objective of this review was to identify studies which have developed such models, determine whether consistent and appropriate methodology was used and whether statistically reliable prognostic models exist.
We searched online databases MEDLINE (1948 onwards), CINAHL Plus (1937 onwards), The Cochrane Library, Web of Science (1898 onwards) and ClinicalTrials.gov, using index terms relating to asthma and prognosis. Data was extracted and assessment of quality was based on GRADE and an early version of PROBAST (Prediction study Risk of Bias Assessment Tool). A meta-analysis of the discrimination and calibration measures was carried out to determine overall performance across models.
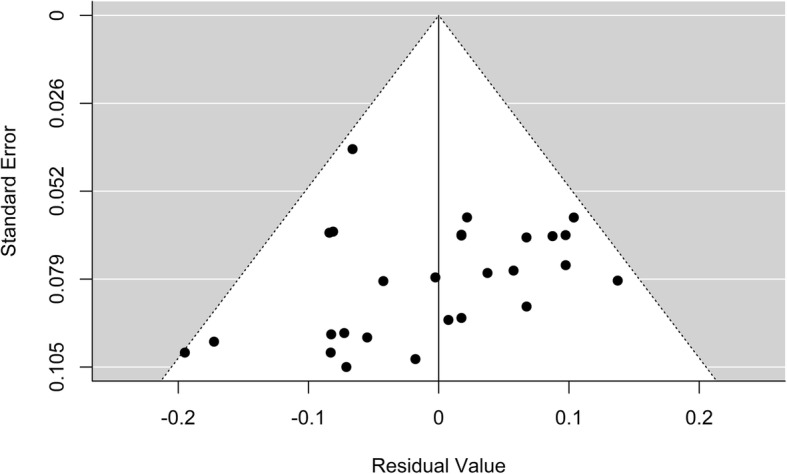
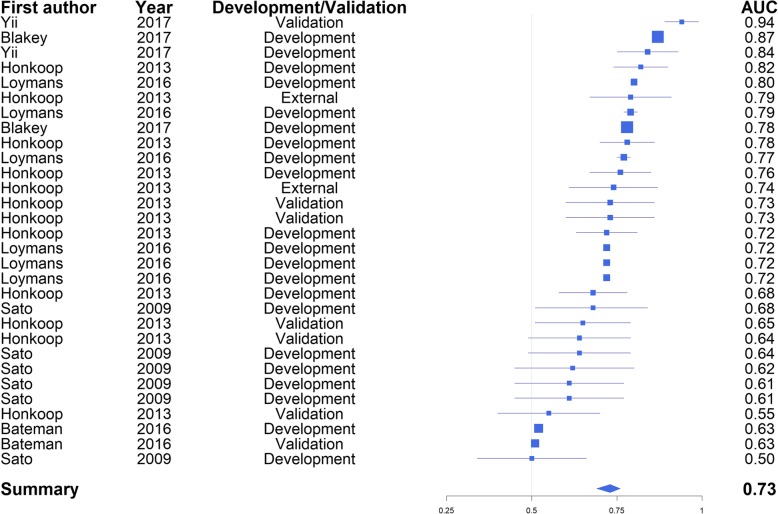
Ten unique prognostic models were identified. GRADE identified moderate risk of bias in two of the studies, but more detailed quality assessment via PROBAST highlighted that most models were developed using highly selected and small datasets, incompletely recorded predictors and outcomes, and incomplete methodology. None of the identified models modelled recurrent exacerbations, instead favouring either presence/absence of an event, or time to first or specified event. Preferred methodologies were logistic regression and Cox proportional hazards regression. The overall pooled c-statistic was 0.77 (95% confidence interval 0.73 to 0.80), though individually some models performed no better than chance. The meta-analysis had an I value of 99.75% indicating a high amount of heterogeneity between studies. The majority of studies were small and did not include internal or external validation, therefore the individual performance measures are likely to be optimistic.
Current prognostic models for asthma exacerbations are heterogeneous in methodology, but reported c-statistics suggest a clinically useful model could be created. Studies were consistent in lacking robust validation and in not modelling serial events. Further research is required with respect to incorporating recurrent events, and to externally validate tools in large representative populations to demonstrate the generalizability of published results.
临床预测模型被广泛用于指导医疗建议和治疗干预。哮喘是全球最常见的慢性疾病之一,其特征是急性恶化。这些恶化在很大程度上是可以预防的,因此人们对在该领域使用临床预测模型感兴趣。本综述的目的是确定已开发此类模型的研究,确定是否使用了一致且适当的方法,以及是否存在统计学上可靠的预后模型。
我们使用与哮喘和预后相关的索引词,在线搜索 MEDLINE(1948 年起)、CINAHL Plus(1937 年起)、The Cochrane Library、Web of Science(1898 年起)和 ClinicalTrials.gov 数据库。提取数据并根据 GRADE 和早期版本的 PROBAST(预测研究风险偏倚评估工具)进行质量评估。对判别和校准测量值进行荟萃分析,以确定模型的整体性能。
确定了 10 个独特的预后模型。GRADE 确定其中 2 项研究存在中度偏倚风险,但通过 PROBAST 进行更详细的质量评估突出表明,大多数模型都是使用高度选择和小数据集、不完全记录的预测因子和结果以及不完整的方法开发的。没有一个确定的模型对复发性恶化进行建模,而是倾向于事件的存在/不存在,或者是首次或特定事件的时间。首选方法是逻辑回归和 Cox 比例风险回归。总体合并的 c 统计量为 0.77(95%置信区间为 0.73 至 0.80),尽管个别模型的表现并不比机会好。荟萃分析的 I 值为 99.75%,表明研究之间存在高度异质性。大多数研究规模较小,且未进行内部或外部验证,因此个别性能指标可能过于乐观。
目前哮喘恶化的预后模型在方法上存在异质性,但报告的 c 统计量表明可以创建一个具有临床意义的模型。研究在缺乏稳健验证和不模拟连续事件方面是一致的。需要进一步研究,包括纳入复发性事件,并在代表性大人群中对外科验证工具进行验证,以证明已发表结果的可推广性。