Li Ka Shing Institute of Health Sciences, Faculty of Medicine, Chinese University of Hong Kong, Hong Kong, SAR, People's Republic of China.
Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular disease, Department of Cardiology, Tianjin Institute of Cardiology, Second Hospital of Tianjin Medical University, Tianjin, 300211, People's Republic of China.
Heart Fail Rev. 2021 Sep;26(5):1141-1150. doi: 10.1007/s10741-020-09927-x.
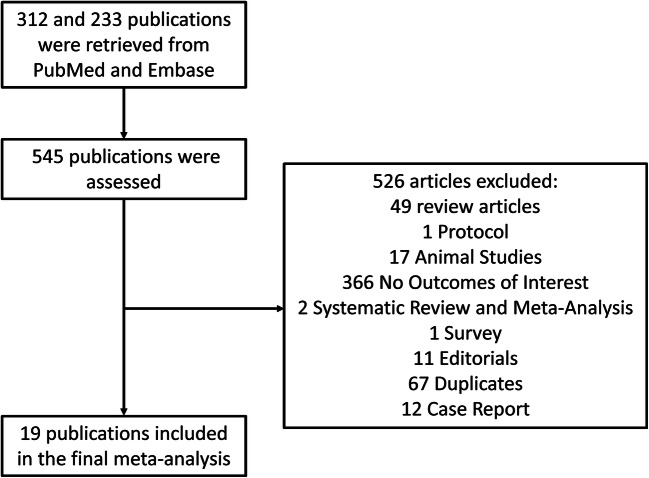
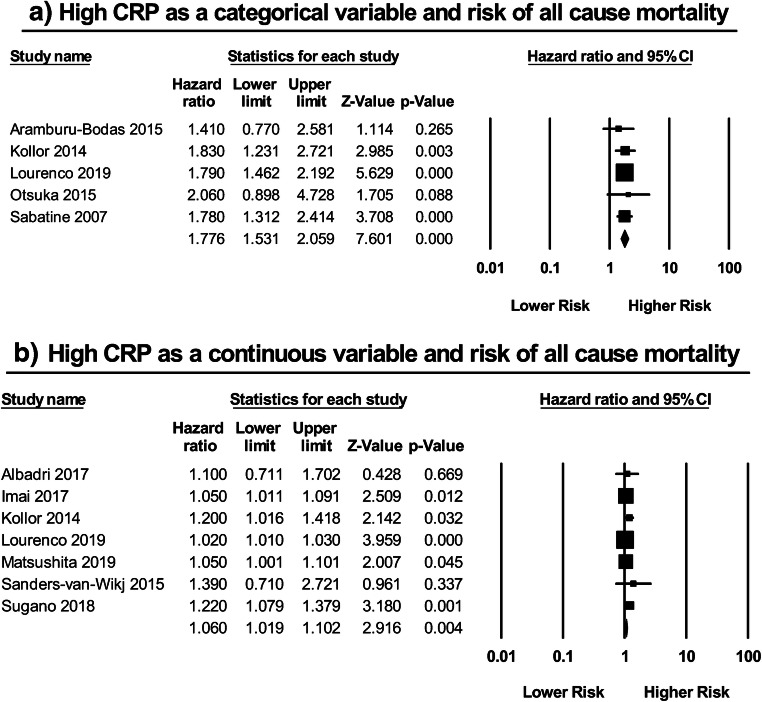
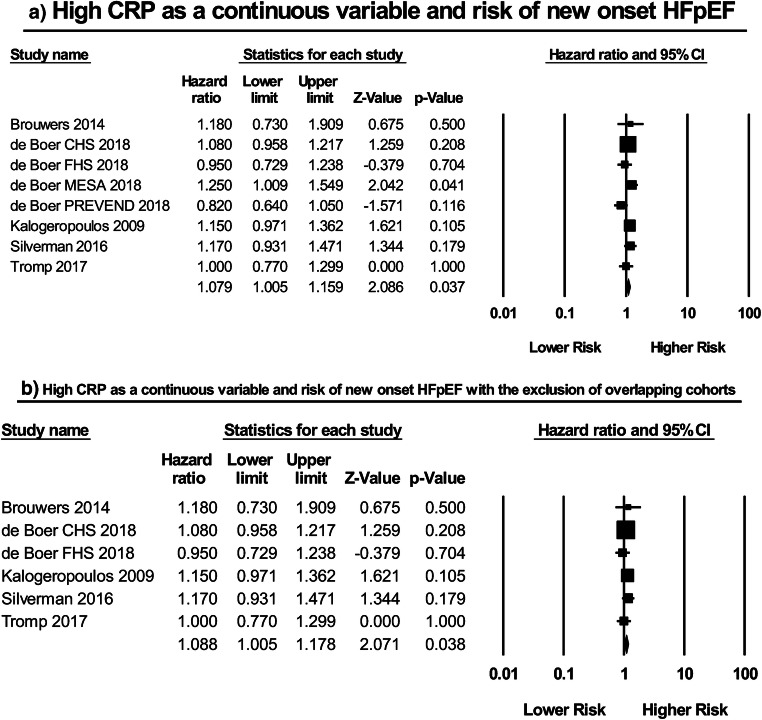
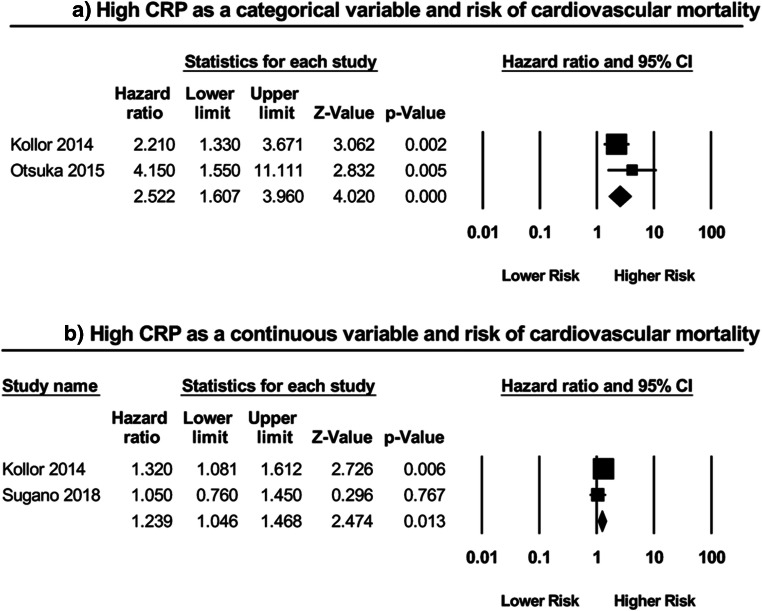
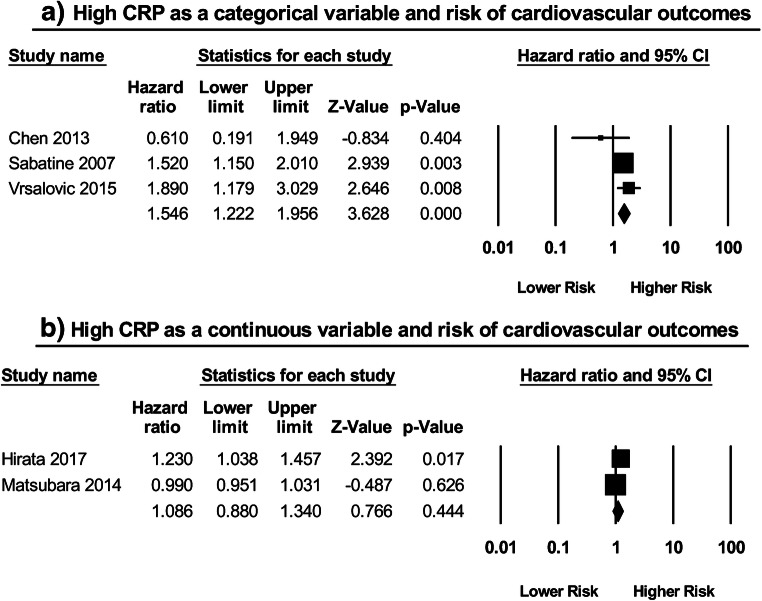
Heart failure (HF) is a major epidemic with rising morbidity and mortality rates that encumber global healthcare systems. While some studies have demonstrated the value of CRP in predicting (i) the development of HFpEF and (ii) long-term clinical outcomes in HFpEF patients, others have shown no such correlation. As a result, we conducted the following systematic review and meta-analysis to assess both the diagnostic and prognostic role of CRP in HFpEF. PubMed and Embase were searched for studies that assess the relationship between CRP and HFpEF using the following search terms: (((C-reactive protein) AND ((preserved ejection fraction) OR (diastolic heart failure))). The search period was from the start of database to August 6, 2019, with no language restrictions. A total of 312 and 233 studies were obtained from PubMed and Embase respectively, from which 19 studies were included. Our meta-analysis demonstrated the value of a high CRP in predicting the development of not only new onset HFpEF (HR: 1.08; 95% CI: 1.00-1.16; P = 0.04; I = 22%), but also an increased risk of cardiovascular mortality when used as a categorical (HR: 2.52; 95% CI: 1.61-3.96; P < 0.0001; I = 19%) or a continuous variable (HR: 1.24; 95% CI: 1.04-1.47; P = 0.01; I = 28%), as well as all-cause mortality when used as a categorical (HR: 1.78; 95% CI: 1.53-2.06; P < 0.00001; I = 0%) or a continuous variable: (HR: 1.06; 95% CI: 1.02-1.06; P = 0.003; I = 61%) in HFpEF patients. CRP can be used as a biomarker to predict the development of HFpEF and long-term clinical outcomes in HFpEF patients, in turn justifying its use as a simple, accessible parameter to guide clinical management in this patient population. However, more prospective studies are still required to not only explore the utility and dynamicity of CRP in HFpEF but also to determine whether risk stratification algorithms incorporating CRP actually provide a material benefit in improving patient prognosis.
心力衰竭(HF)是一种发病率和死亡率不断上升的主要流行病,给全球医疗系统带来了负担。虽然一些研究已经证明了 CRP 在预测(i)HFpEF 的发展和(ii)HFpEF 患者的长期临床结局方面的价值,但其他研究并未显示出这种相关性。因此,我们进行了这项系统评价和荟萃分析,以评估 CRP 在 HFpEF 中的诊断和预后作用。我们使用以下搜索词在 PubMed 和 Embase 上搜索评估 CRP 与 HFpEF 之间关系的研究:(((C 反应蛋白)和((保留射血分数)或(舒张性心力衰竭)))。搜索期从数据库开始到 2019 年 8 月 6 日,没有语言限制。从 PubMed 和 Embase 分别获得了 312 项和 233 项研究,其中纳入了 19 项研究。我们的荟萃分析表明,高 CRP 不仅可预测新发 HFpEF 的发展(HR:1.08;95%CI:1.00-1.16;P=0.04;I=22%),而且当用作分类变量(HR:2.52;95%CI:1.61-3.96;P<0.0001;I=19%)或连续变量(HR:1.24;95%CI:1.04-1.47;P=0.01;I=28%)时,心血管死亡率也会增加,当用作分类变量(HR:1.78;95%CI:1.53-2.06;P<0.00001;I=0%)或连续变量时,全因死亡率也会增加:(HR:1.06;95%CI:1.02-1.06;P=0.003;I=61%)HFpEF 患者。CRP 可作为预测 HFpEF 发展和 HFpEF 患者长期临床结局的生物标志物,这证明了其作为一种简单、可获得的参数来指导该患者人群的临床管理的合理性。然而,仍需要更多的前瞻性研究来探索 CRP 在 HFpEF 中的效用和动态变化,以及确定纳入 CRP 的风险分层算法是否确实能在改善患者预后方面带来实质性的益处。