Department of General Paediatrics, Erasmus MC - Sophia Children's Hospital, P.O. Box 2060, 3000 CB, Rotterdam, The Netherlands.
Paediatric Emergency Department, Cruces University Hospital, Plaza de Cruces s/n, 48903, Bilbao, Spain.
Eur J Pediatr. 2020 Jul;179(7):1097-1106. doi: 10.1007/s00431-020-03601-y. Epub 2020 Feb 8.
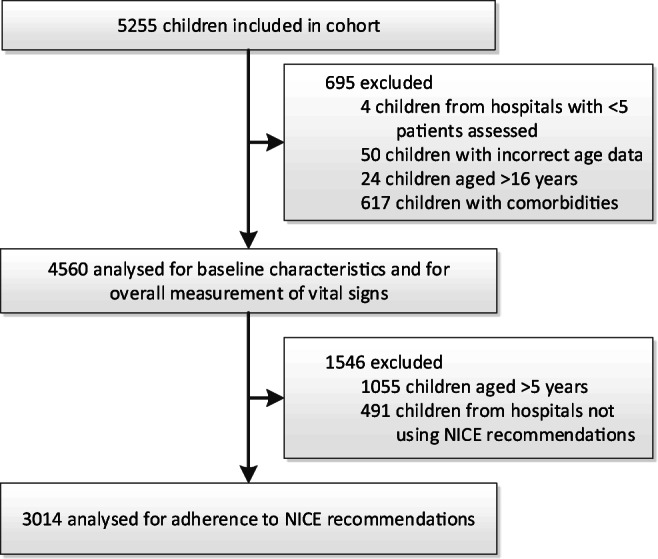
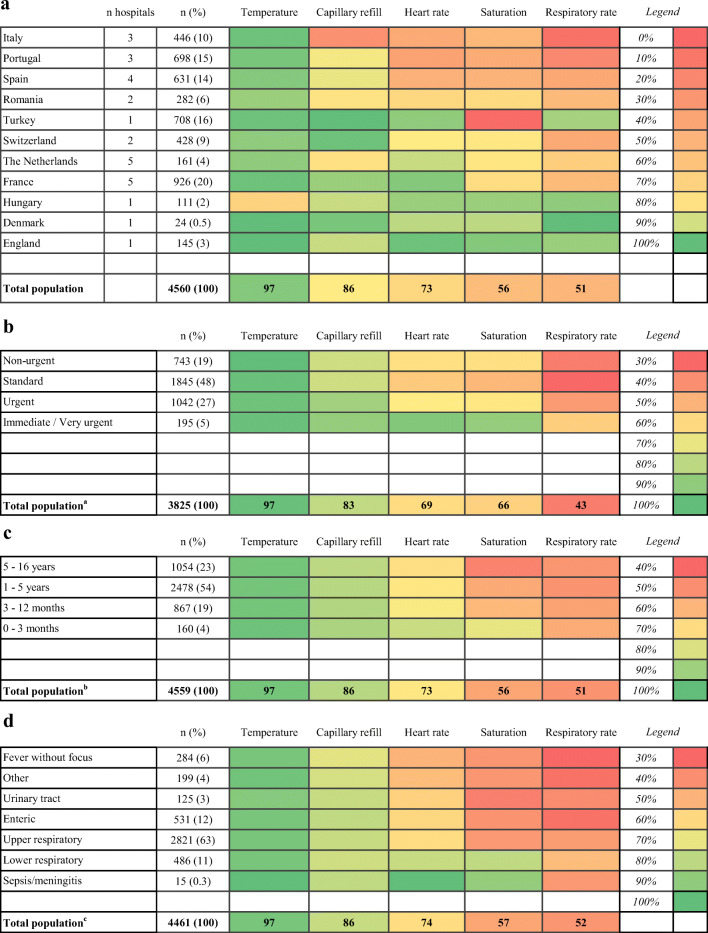
Vital signs can help clinicians identify children at risk of serious illness. The NICE guideline for fever in under-fives recommends a routine measurement of temperature, heart rate, capillary refill and respiratory rate in all febrile children visiting the emergency department (ED). This study aims to evaluate the measurement of paediatric vital signs in European EDs, with specific attention to adherence to this NICE guideline recommendation. In a prospective observational study, we included 4560 febrile children under 16 years from the ED of 28 hospitals in 11 European countries (2014-2016). Hospitals were academic (n = 17), teaching (n = 10) and non-teaching (n = 1) and ranged in annual paediatric ED visits from 2700 to 88,000. Fifty-four percent were male, their median age was 2.4 years (IQR 1.1-4.7). Temperature was measured most frequently (97%), followed by capillary refill (86%), heart rate (73%), saturation (56%) and respiratory rate (51%). In children under five (n = 3505), a complete measurement of the four NICE-recommended vital signs was performed in 48% of patients. Children under 1 year of age, those with an urgent triage level and with respiratory infections had a higher likelihood of undergoing complete measurements. After adjustment for these factors, variability between countries remained. Conclusion: Measuring vital signs in children with fever in the ED occurs with a high degree of practice variation between different European hospitals, and adherence to the NICE recommendation is moderate. Our study is essential as a benchmark for current clinical practice, in order to tailor implementation strategies to different European settings.What is Known:• Vital signs can quickly provide information on disease severity in children in the emergency department (ED), and the NICE guideline for fever in under-fives recommends to routinely measure temperature, heart rate, capillary refill and respiratory rate.• Data regarding measurement of vital signs in routine practice across European EDs is currently unavailable.What is New:• Measurement of vital signs in febrile children is highly variable across European EDs and across patient subgroups, and compliance to the NICE recommendation is <50%.• Children under 1 year of age, those with an urgent triage level and with respiratory infections had a higher likelihood of undergoing complete measurements.
生命体征有助于临床医生识别有严重疾病风险的儿童。NICE 关于五岁以下儿童发热的指南建议,所有发热儿童在急诊科就诊时常规测量体温、心率、毛细血管再充盈时间和呼吸频率。本研究旨在评估欧洲急诊科儿科生命体征的测量情况,特别关注对这一 NICE 指南建议的依从性。在一项前瞻性观察研究中,我们纳入了来自欧洲 11 个国家 28 家医院急诊科的 4560 名发热儿童(2014-2016 年)。医院为学术型(n=17)、教学型(n=10)和非教学型(n=1),年儿科急诊就诊量为 2700 至 88000 人不等。54%为男性,中位年龄为 2.4 岁(IQR 1.1-4.7)。最常测量体温(97%),其次是毛细血管再充盈(86%)、心率(73%)、饱和度(56%)和呼吸频率(51%)。在五岁以下儿童(n=3505)中,48%的患者进行了四项 NICE 推荐的生命体征的完整测量。年龄在 1 岁以下、紧急分诊级别和患有呼吸道感染的儿童更有可能进行完整的测量。在调整这些因素后,国家间的差异仍然存在。结论:在欧洲不同医院的急诊科,对发热儿童进行生命体征测量的做法存在很大差异,对 NICE 建议的依从性中等。我们的研究对于当前临床实践来说是一个基准,以便针对不同的欧洲环境制定实施策略。已知:•生命体征可以快速提供急诊科儿童疾病严重程度的信息,NICE 关于五岁以下儿童发热的指南建议常规测量体温、心率、毛细血管再充盈时间和呼吸频率。•目前尚无关于欧洲急诊科常规实践中生命体征测量的数据。新发现:•在欧洲急诊科,发热儿童的生命体征测量差异很大,而且差异很大,而且对 NICE 建议的依从性<50%。•年龄在 1 岁以下、紧急分诊级别和患有呼吸道感染的儿童更有可能进行完整的测量。