Division of Pediatric Pulmonology, Allergology and Endocrinology, Department of Pediatrics and Adolescent Medicine, Medical University Vienna, Waehringer Guertel 18-20, 1090, Vienna, Austria.
Center for Medical Statistics, Informatics and Intelligent Systems, Institute of Medical Statistics, Medical University Vienna, Spitalgasse 23, 1090, Vienna, Austria.
Eur J Pediatr. 2022 Nov;181(11):3831-3838. doi: 10.1007/s00431-022-04594-6. Epub 2022 Aug 27.
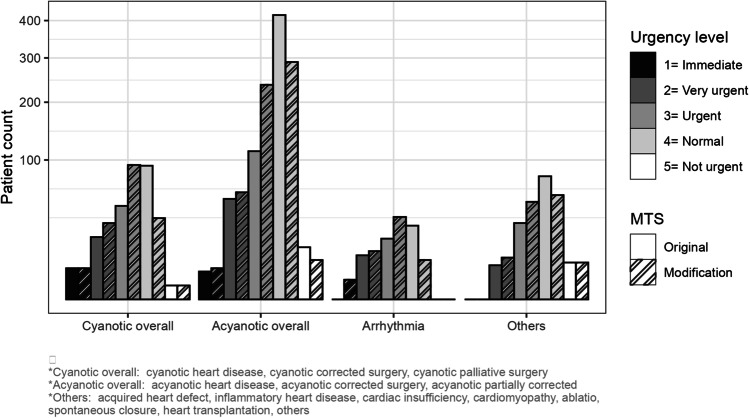
This study is a prospective evaluation of the validity of a Manchester triage system (MTS) modification for detecting under-triaged pediatric patients with congenital heart disease (CHD). Children with CHD visiting the emergency unit of the Department of Pediatrics and Adolescent Medicine, University Hospital Vienna in 2014 were included. The MTS modification updated the prioritization of patients with complex syndromic diseases, specific symptoms related to chronic diseases, decreased general condition (DGC), profound language impairment, unknown medical history, or special needs. A four-level outcome severity index based on diagnostic and therapeutic interventions, admission to hospital, and follow-up strategies was defined as a reference standard for the correct clinical classification of the MTS urgency level. Of the 19,264 included children, 940 had CHD. Of this group, 266 fulfilled the inclusion criteria for the modified triage method. The MTS modification was significantly more often applied in under-triaged (65.9%) than correctly or over-triaged (25%) children with CHD (p-value χ test < 0.0001, OR 5.848, 95% CI: 3.636-9.6).
The MTS urgency level upgrade modification could reduce under-triage in children with CHD. Applying a safety strategy concept to the MTS could mitigate under-triage in such a high-risk patient group.
• The Manchester triage system is considered to be valid and reliable but tends to over-triage. • A study by Seiger et al. showed poor performance in children with chronic illnesses, especially in children with cardiovascular diseases.
• The MTS modification with one urgency level upgrade could decrease under-triage in children with congenital heart disease. • As reference standard a four level outcome severity index (OSI) was established to include diagnostic investigations, medical interventions, hospital admission or follow up visits in the assessment.
本研究旨在评估曼彻斯特分诊系统(MTS)改良版用于检测先天性心脏病(CHD)患儿分诊不足的有效性。
纳入 2014 年在维也纳大学儿童医院儿科和青少年医学系急诊就诊的 CHD 患儿。MTS 改良版更新了复杂综合征患儿、与慢性疾病相关的特定症状、一般情况较差(DGC)、严重语言障碍、未知病史或特殊需求患儿的优先分诊顺序。基于诊断和治疗干预、住院和随访策略的四级结局严重程度指数被定义为 MTS 紧急程度正确临床分类的参考标准。
在纳入的 19264 例患儿中,940 例患有 CHD。其中,266 例患儿符合改良分诊方法的纳入标准。MTS 改良版在分诊不足(65.9%)的 CHD 患儿中比正确或过度分诊(25%)更常应用(χ²检验,p<0.0001,OR 5.848,95%CI:3.636-9.6)。
MTS 紧急程度升级改良版可降低 CHD 患儿分诊不足的发生率。将安全策略概念应用于 MTS 可减少此类高风险患儿群体的分诊不足。
曼彻斯特分诊系统被认为是有效且可靠的,但存在过度分诊的趋势。Seiger 等人的研究表明,该系统在慢性疾病患儿中表现不佳,尤其是心血管疾病患儿。
MTS 改良版通过一级紧急程度升级可降低 CHD 患儿的分诊不足率。建立四级结局严重程度指数(OSI)作为参考标准,以评估诊断性检查、医疗干预、住院或随访就诊。