Piecha Felix, Radunski Ulf K, Ozga Ann-Kathrin, Steins David, Drolz Andreas, Horvatits Thomas, Spink Clemens, Ittrich Harald, Benten Daniel, Lohse Ansgar W, Sinning Christoph, Kluwe Johannes
I. Department of Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Department of General and Interventional Cardiology, University Heart Center Hamburg-Eppendorf, Hamburg, Germany.
JHEP Rep. 2019 May 10;1(2):90-98. doi: 10.1016/j.jhepr.2019.04.001. eCollection 2019 Aug.
BACKGROUND & AIMS: Refractory ascites is the main reason for the implantation of a transjugular intrahepatic portosystemic shunt (TIPS) in liver cirrhosis, but ascites control by TIPS fails in a relevant proportion of cases. Here, we investigated whether routine parameters pre-TIPS can predict persistent ascites after TIPS implantation and whether persistent ascites predicts long-term clinical outcome.
A detailed retrospective analysis of 128 patients receiving expanded polytetrafluoroethylene-covered stents for the treatment of refractory ascites was performed. Persistent ascites post-TIPS was defined as the prolonged need for paracentesis >3 months after TIPS. The influence of demographics, laboratory results, pre-TIPS heart and liver ultrasound results, and invasive hemodynamic parameters on persistent ascites was evaluated by univariable and multivariable logistic regression. Predictors of the composite endpoint liver transplantation/death were analyzed using a multivariable Cox regression.
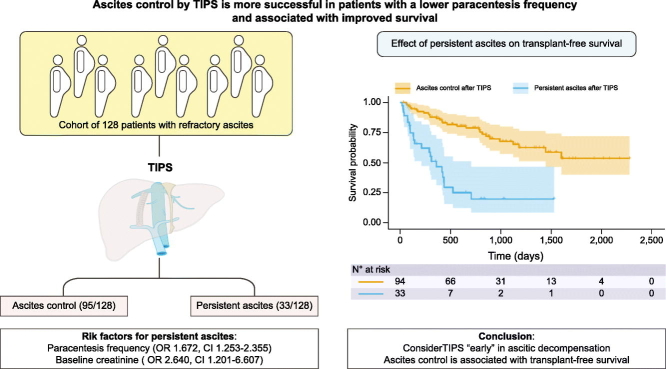
Ascites control post-TIPS was achieved in 95/128 patients (74%), whereas ascites remained persistent in 33/128 cases (26%). On multivariable analysis, a lower paracentesis frequency pre-TIPS (odds ratio 1.672; 95% CI 1.253-2.355) and lower baseline creatinine levels (odds ratio 2.640; CI 1.201-6.607) were associated with ascites control. Patients with persistent ascites post-TIPS had and impaired transplant-free survival (median 10.0 25.8 months), for which persistent ascites was the only independent predictor (hazard ratio 5.654; CI 3.019-10.59).
TIPS-placement in patients with lower paracentesis frequency and creatinine levels is associated with superior ascites control. Thus, TIPS implantation should be considered in moderate decompensation and not as a last resort. Persistent ascites post-TIPS seems to be the only predictor of liver transplantation and death.
The insertion of a transjugular intrahepatic portosystemic shunt (TIPS) in patients with refractory ascites should be considered in patients with moderate decompensation and not as a last resort, as lower paracentesis frequency and creatinine levels pre-TIPS are associated with superior ascites control. In turn, failure to control ascites seems to be the only predictor of liver transplantation and death.
顽固性腹水是肝硬化患者行经颈静脉肝内门体分流术(TIPS)的主要原因,但在相当一部分病例中,TIPS对腹水的控制效果不佳。在此,我们研究了TIPS术前的常规参数是否能预测TIPS植入术后腹水持续存在的情况,以及腹水持续存在是否能预测长期临床结局。
对128例接受膨体聚四氟乙烯覆膜支架治疗顽固性腹水的患者进行了详细的回顾性分析。TIPS术后腹水持续存在定义为TIPS术后需要反复进行腹腔穿刺>3个月。通过单变量和多变量逻辑回归评估人口统计学、实验室检查结果、TIPS术前心脏和肝脏超声检查结果以及有创血流动力学参数对腹水持续存在的影响。使用多变量Cox回归分析肝移植/死亡复合终点的预测因素。
128例患者中有95例(74%)TIPS术后腹水得到控制,而128例中有33例(26%)腹水持续存在。多变量分析显示,TIPS术前腹腔穿刺频率较低(比值比1.672;95%置信区间1.253 - 2.355)和基线肌酐水平较低(比值比2.640;置信区间1.201 - 6.607)与腹水控制相关。TIPS术后腹水持续存在的患者无移植生存期受损(中位数10.0对25.8个月),其中腹水持续存在是唯一的独立预测因素(风险比5.654;置信区间3.019 - 10.59)。
腹腔穿刺频率和肌酐水平较低的患者行TIPS治疗与更好的腹水控制相关。因此,TIPS植入应在中度失代偿期考虑,而不应作为最后的手段。TIPS术后腹水持续存在似乎是肝移植和死亡的唯一预测因素。
对于顽固性腹水患者,TIPS植入应在中度失代偿期考虑,而不应作为最后的手段,因为TIPS术前腹腔穿刺频率和肌酐水平较低与更好的腹水控制相关。反过来,腹水控制不佳似乎是肝移植和死亡的唯一预测因素。