Department of Neurology, Anschutz Medical Campus, University of Colorado, Denver, Aurora.
Now with Department of Neurology, University of Rochester Medical Center, Rochester, New York.
JAMA Neurol. 2020 May 1;77(5):551-560. doi: 10.1001/jamaneurol.2019.4992.
Parkinson disease and related disorders (PDRD) have consequences for quality of life (QoL) and are the 14th leading cause of death in the United States. Despite growing interest in palliative care (PC) for persons with PDRD, few studies are available supporting its effectiveness.
To determine if outpatient PC is associated with improvements in patient-centered outcomes compared with standard care among patients with PDRD and their caregivers.
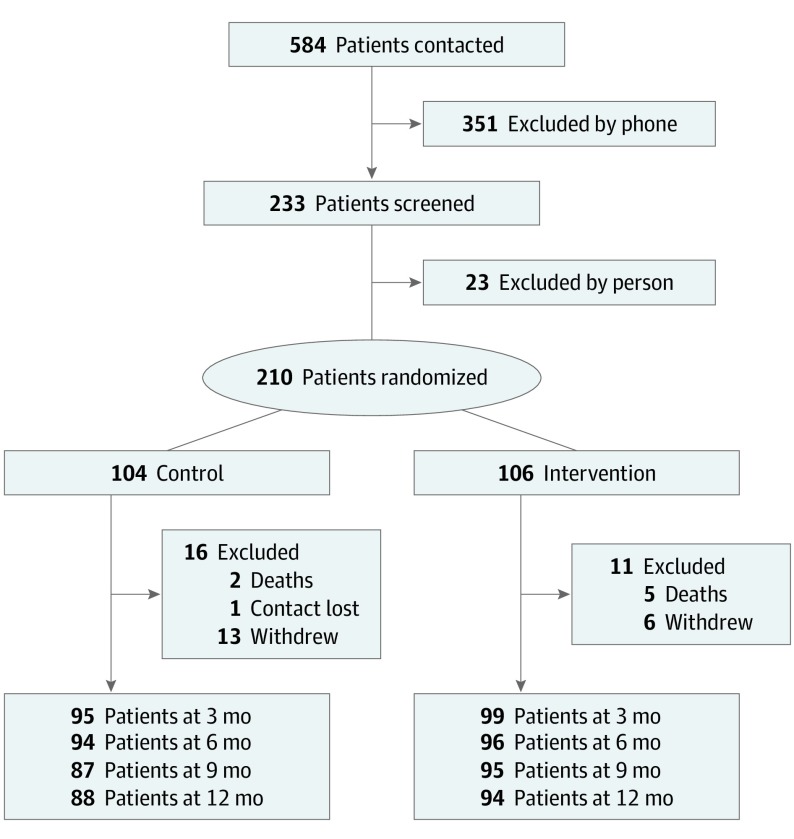
DESIGN, SETTING, AND PARTICIPANTS: This randomized clinical trial enrolled participants at 3 academic tertiary care centers between November 1, 2015, and September 30, 2017, and followed them up for 1 year. A total of 584 persons with PDRD were referred to the study. Of those, 351 persons were excluded by phone and 23 were excluded during in-person screenings. Patients were eligible to participate if they had PDRD and moderate to high PC needs. Patients were excluded if they had urgent PC needs, another diagnosis meriting PC, were already receiving PC, or were unable or unwilling to follow the study protocol. Enrolled participants were assigned to receive standard care plus outpatient integrated PC or standard care alone. Data were analyzed between November 1, 2018, and December 9, 2019.
Outpatient integrated PC administered by a neurologist, social worker, chaplain, and nurse using PC checklists, with guidance and selective involvement from a palliative medicine specialist. Standard care was provided by a neurologist and a primary care practitioner.
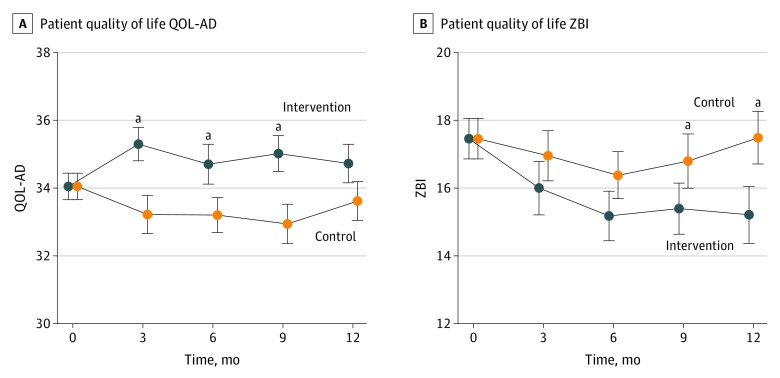
The primary outcomes were the differences in patient quality of life (QoL; measured by the Quality of Life in Alzheimer Disease scale) and caregiver burden (measured by the Zarit Burden Interview) between the PC intervention and standard care groups at 6 months.
A total of 210 patients with PDRD (135 men [64.3%]; mean [SD] age, 70.1 [8.2] years) and 175 caregivers (128 women [73.1%]; mean [SD] age, 66.1 [11.1] years) were enrolled in the study; 193 participants (91.9%) were white and non-Hispanic. Compared with participants receiving standard care alone at 6 months, participants receiving the PC intervention had better QoL (mean [SD], 0.66 [5.5] improvement vs 0.84 [4.2] worsening; treatment effect estimate, 1.87; 95% CI, 0.47-3.27; P = .009). No significant difference was observed in caregiver burden (mean [SD], 2.3 [5.0] improvement vs 1.2 [5.6] improvement in the standard care group; treatment effect estimate, -1.62; 95% CI, -3.32 to 0.09; P = .06). Other significant differences favoring the PC intervention included nonmotor symptom burden, motor symptom severity, completion of advance directives, caregiver anxiety, and caregiver burden at 12 months. No outcomes favored standard care alone. Secondary analyses suggested that benefits were greater for persons with higher PC needs.
Outpatient PC is associated with benefits among patients with PDRD compared with standard care alone. This study supports efforts to integrate PC into PDRD care. The lack of diversity and implementation of PC at experienced centers suggests a need for implementation research in other populations and care settings.
ClinicalTrials.gov Identifier: NCT02533921.
重要性:帕金森病和相关疾病(PDRD)会对生活质量(QoL)产生影响,是美国第 14 大死因。尽管人们对 PDRD 患者的姑息治疗(PC)越来越感兴趣,但很少有研究支持其有效性。
目的:确定与标准护理相比,门诊 PC 是否能改善 PDRD 患者及其护理人员的以患者为中心的结局。
设计、地点和参与者:这项随机临床试验于 2015 年 11 月 1 日至 2017 年 9 月 30 日在 3 个学术三级护理中心招募参与者,并随访 1 年。共有 584 名 PDRD 患者被推荐参加该研究。其中,通过电话排除了 351 人,在现场筛查中排除了 23 人。如果患者有 PDRD 且有中度到高度 PC 需求,则有资格参加研究。如果患者有紧急 PC 需求、有其他需要 PC 的诊断、正在接受 PC 或无法或不愿意遵守研究方案,则将其排除在外。纳入的参与者被分配接受标准护理加门诊综合 PC 或标准护理单独治疗。数据分析于 2018 年 11 月 1 日至 2019 年 12 月 9 日进行。
干预措施:由神经科医生、社会工作者、牧师和护士使用 PC 检查表进行门诊综合 PC,由姑息医学专家提供指导和选择性参与。标准护理由神经科医生和初级保健医生提供。
主要结果和措施:主要结果是在 6 个月时,PC 干预组和标准护理组之间患者生活质量(通过阿尔茨海默病生活质量量表测量)和护理人员负担(通过 Zarit 负担量表测量)的差异。
结果:共有 210 名 PDRD 患者(135 名男性[64.3%];平均[SD]年龄 70.1[8.2]岁)和 175 名护理人员(128 名女性[73.1%];平均[SD]年龄 66.1[11.1]岁)入组研究;193 名参与者(91.9%)为白人且非西班牙裔。与单独接受标准护理的参与者相比,接受 PC 干预的参与者生活质量更好(平均[SD],0.66[5.5]改善与 0.84[4.2]恶化;治疗效果估计值为 1.87;95%CI,0.47-3.27;P=0.009)。在护理人员负担方面没有观察到显著差异(平均[SD],2.3[5.0]改善与标准护理组 1.2[5.6]改善;治疗效果估计值为-1.62;95%CI,-3.32 至 0.09;P=0.06)。其他有利于 PC 干预的显著差异包括非运动症状负担、运动症状严重程度、完成预先指示、护理人员焦虑和 12 个月时的护理人员负担。没有结果有利于单独的标准护理。次要分析表明,对于 PC 需求较高的患者,获益更大。
结论和相关性:与单独的标准护理相比,门诊 PC 与 PDRD 患者的获益相关。本研究支持将 PC 纳入 PDRD 护理的努力。缺乏多样性和在经验丰富的中心实施 PC 表明,需要在其他人群和护理环境中进行实施研究。
试验注册:ClinicalTrials.gov 标识符:NCT02533921。