University Hospital for Children and Adolescents, Division for Stem Cell Transplantation and Immunology, Goethe University Frankfurt am Main, 60528 Frankfurt am Main, Germany.
Institute for Transfusion Medicine and Immunohaematology, German Red Cross Blood Donor Service Baden-Württemberg-Hessen GmbH, Goethe University Hospital, 60528 Frankfurt am Main, Germany.
Cells. 2020 Feb 12;9(2):431. doi: 10.3390/cells9020431.
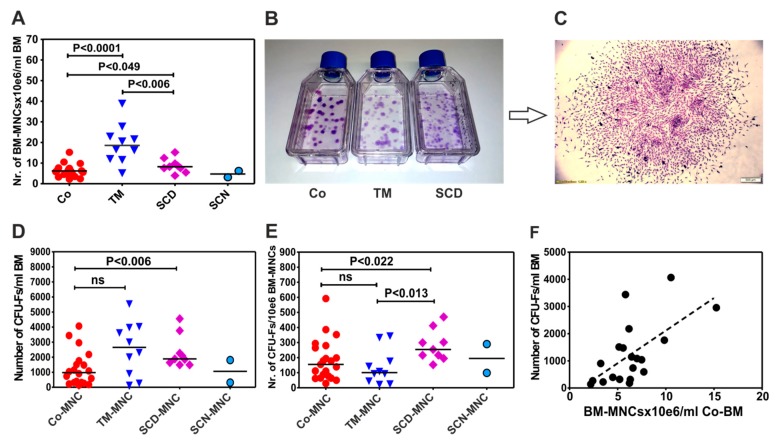
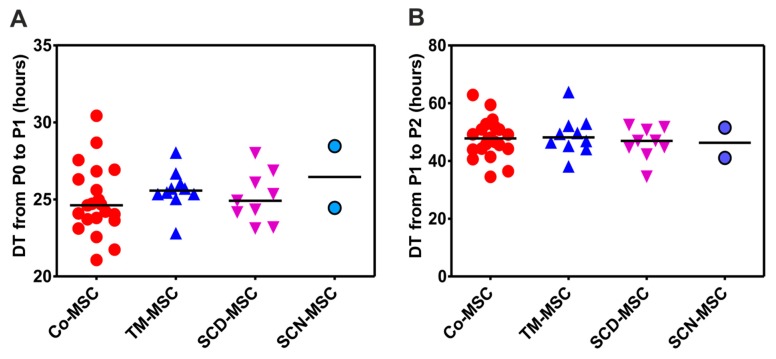
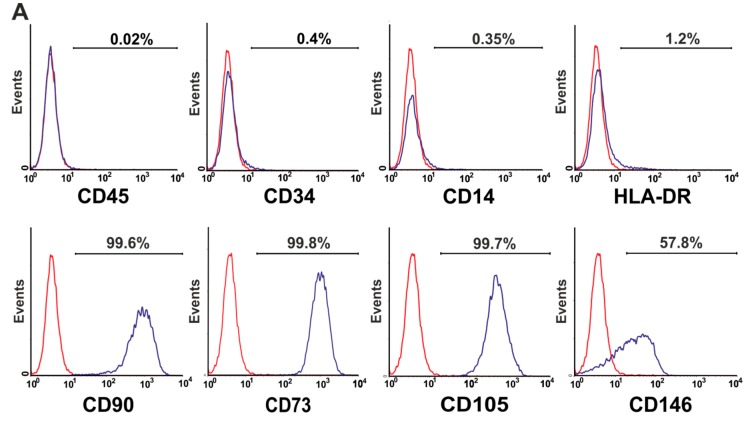
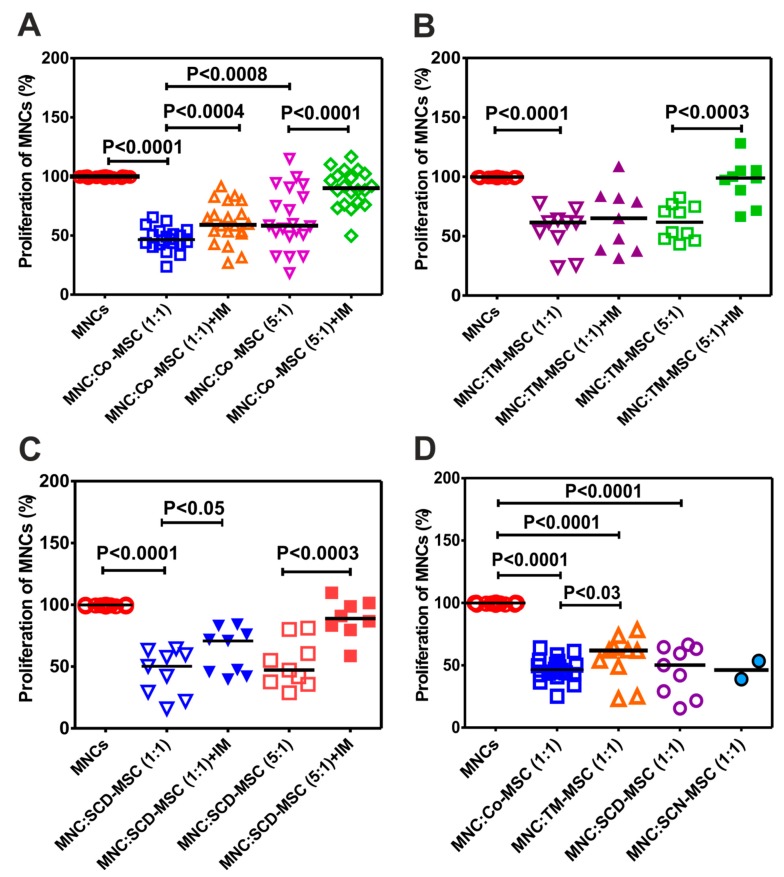
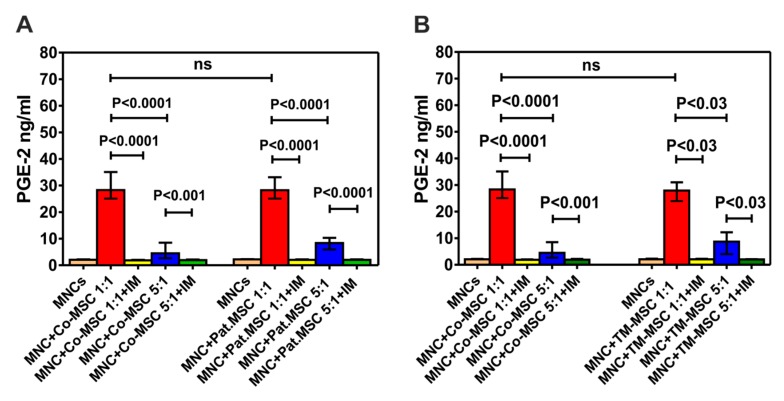
As the biology of mesenchymal stromal cells (MSCs) in patients with non-malignant hematological diseases (NMHD) is poorly understood, in the current study we performed a basic characterization of the phenotype and functional activity of NMHD-MSCs. Bone marrow (BM) of patients with thalassemia major (TM) possessed a significantly higher number of nucleated cells (BM-MNCs)/mL BM than healthy donors ( < 0.0001), which however did not result in a higher number of colony forming units-fibroblast (CFU-F) per milliliter BM. In contrast, from 1 × 10 BM-MNCs of patients with sickle cell disease (SCD) were generated significantly more CFU-Fs than from TM-BM-MNCs ( < 0.013) and control group ( < 0.02). In addition, NMHD-MSCs expressed significantly lower levels of CD146 molecule, demonstrated an equal proliferation potential and differentiated along three lineages (osteoblasts, chondrocytes and adipocytes) as healthy donors' MSCs, with exception of TM-MSCs which differentiated weakly in adipocytes. In contrast to other NMHD-MSCs and healthy donors' MSCs, TM-MSCs demonstrated an impaired in vitro immunosuppressive potential, either. Noteworthy, the majority of the immunosuppressive effect of NMHD-MSCs was mediated through prostaglandin-E2 (PGE2), because indomethacin (an inhibitor of PGE2 synthesis) was able to significantly reverse this effect. Our results indicate therefore that NMHD-MSCs, except TM-MSCs, may be used as an autologous cell-based therapy for post-transplant complications such as graft failure, graft-versus-host disease (GvHD) and osteonecrosis.
由于非恶性血液病(NMHD)患者间充质基质细胞(MSC)的生物学特性尚未完全了解,在本研究中,我们对 NMHD-MSC 的表型和功能活性进行了基本特征描述。与健康供体相比(<0.0001),重型地中海贫血(TM)患者的骨髓(BM)中的有核细胞(BM-MNC)/mL BM 数量明显更高,但这并未导致每毫升 BM 中的集落形成单位-成纤维细胞(CFU-F)数量更高。相比之下,从 1×10 的 SCD 患者的 BM-MNC 中产生的 CFU-F 数量明显多于 TM-BM-MNC(<0.013)和对照组(<0.02)。此外,NMHD-MSC 表达的 CD146 分子水平明显较低,其增殖潜能相同,并沿着三个谱系(成骨细胞、软骨细胞和脂肪细胞)分化,与健康供体的 MSC 相同,但 TM-MSC 分化为脂肪细胞的能力较弱。与其他 NMHD-MSC 和健康供体的 MSC 不同,TM-MSC 的体外免疫抑制潜能也受损。值得注意的是,NMHD-MSC 的大部分免疫抑制作用是通过前列腺素 E2(PGE2)介导的,因为吲哚美辛(PGE2 合成抑制剂)能够显著逆转这种作用。因此,我们的研究结果表明,除 TM-MSC 外,NMHD-MSC 可作为自体细胞疗法,用于治疗移植后并发症,如移植物失败、移植物抗宿主病(GvHD)和骨坏死。