Brigham and Women's Hospital, Boston, Massachusetts (D.H.S., R.J.G., E.W.K., F.L., C.C., J.C., C.X., J.M., N.B., P.F.D., B.M.E., A.D.P., S.P.H., M.M., D.A.R., S.Y.R., A.R., J.A.S., J.S., D.H.S., S.K.T., K.M.V., N.P.P., P.M.R.).
Hospital for Special Surgery, New York, New York (M.B.).
Ann Intern Med. 2020 Mar 17;172(6):369-380. doi: 10.7326/M19-3369. Epub 2020 Feb 18.
Low-dose methotrexate (LD-MTX) is the most commonly used drug for systemic rheumatic diseases worldwide and is the recommended first-line agent for rheumatoid arthritis. Despite extensive clinical use for more than 30 years, few data on adverse event (AE) rates derive from randomized, placebo-controlled trials, where both causality and magnitude of risk can be inferred.
To investigate AE rates, risk, and risk differences comparing LD-MTX versus placebo.
Prespecified secondary analyses of a double-blind, placebo-controlled, randomized trial. (ClinicalTrials.gov: NCT01594333).
North America.
Adults with known cardiovascular disease and diabetes or metabolic syndrome.
Random allocation to LD-MTX (≤20 mg/wk) or placebo. All participants received folic acid, 1 mg/d, 6 days per week.
Risks for specific AEs of interest, as well as for all AEs, were compared across treatment groups after blinded adjudication.
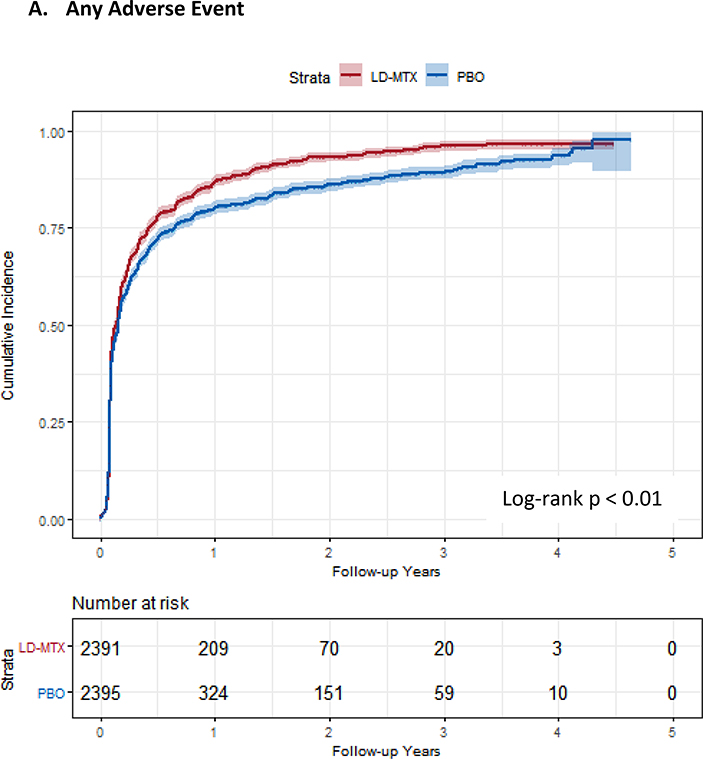
After an active run-in period, 6158 patients were enrolled and 4786 randomly assigned to a group; median follow-up was 23 months and median dosage 15 mg/wk. Among the randomly assigned participants, 81.2% were male, median age was 65.7 years, and median body mass index was 31.5 kg/m2. Of 2391 participants assigned to LD-MTX, 2080 (87.0%) had an AE of interest, compared with 1951 of 2395 (81.5%) assigned to placebo (hazard ratio [HR], 1.17 [95% CI, 1.10 to 1.25]). The relative hazards of gastrointestinal (HR, 1.91 [CI, 1.75 to 2.10]), pulmonary (HR, 1.52 [CI, 1.16 to 1.98]), infectious (HR, 1.15 [CI, 1.01 to 1.30]), and hematologic (HR, 1.15 [CI, 1.07 to 1.23]) AEs were elevated for LD-MTX versus placebo. With the exception of increased risk for skin cancer (HR, 2.05 [CI, 1.28 to 3.28]), the treatment groups did not differ in risk for other cancer or mucocutaneous, neuropsychiatric, or musculoskeletal AEs. Renal AEs were reduced in the LD-MTX group (HR, 0.85 [CI, 0.78 to 0.93]).
The trial was done in patients without rheumatic disease who tolerated LD-MTX during an active run-in period.
Use of LD-MTX was associated with small to moderate elevations in risks for skin cancer and gastrointestinal, infectious, pulmonary, and hematologic AEs, whereas renal AEs were decreased.
National Institutes of Health.
低剂量甲氨蝶呤(LD-MTX)是全球范围内治疗系统性风湿疾病最常用的药物,也是类风湿关节炎的首选一线药物。尽管它已经被广泛应用了 30 多年,但很少有数据来自随机、安慰剂对照试验,这些试验可以推断出不良反应(AE)的因果关系和风险程度。
调查 LD-MTX 与安慰剂相比的不良反应发生率、风险和风险差异。
双盲、安慰剂对照、随机试验的预先指定的次要分析。(ClinicalTrials.gov:NCT01594333)。
北美。
患有已知心血管疾病和糖尿病或代谢综合征的成年人。
随机分配至 LD-MTX(≤20mg/周)或安慰剂。所有参与者均接受叶酸,每天 1mg,每周 6 天。
经过盲法裁决后,比较治疗组之间特定感兴趣的不良反应以及所有不良反应的风险。
在一个主动的导入期后,共纳入了 6158 名患者,其中 4786 名被随机分组;中位随访时间为 23 个月,中位剂量为 15mg/周。在随机分配的参与者中,81.2%为男性,中位年龄为 65.7 岁,中位体重指数为 31.5kg/m2。在 2391 名被分配至 LD-MTX 的参与者中,有 2080 名(87.0%)发生了感兴趣的不良反应,而在 2395 名被分配至安慰剂的参与者中,有 1951 名(81.5%)发生了不良反应(风险比[HR],1.17[95%CI,1.10 至 1.25])。与安慰剂相比,胃肠道(HR,1.91[CI,1.75 至 2.10])、肺部(HR,1.52[CI,1.16 至 1.98])、感染性(HR,1.15[CI,1.01 至 1.30])和血液学(HR,1.15[CI,1.07 至 1.23])不良反应的风险升高。除皮肤癌风险增加(HR,2.05[CI,1.28 至 3.28])外,两组在其他癌症或黏膜皮肤、神经精神或肌肉骨骼不良反应的风险方面没有差异。LD-MTX 组的肾脏不良反应减少(HR,0.85[CI,0.78 至 0.93])。
该试验是在没有风湿性疾病且在主动导入期内耐受 LD-MTX 的患者中进行的。
LD-MTX 的使用与皮肤癌和胃肠道、感染、肺部和血液学不良反应的风险小到中度升高相关,而肾脏不良反应则减少。
美国国立卫生研究院。