From the Institute for Experimental Medical Research, Oslo University Hospital (K.T., M.F., M.L., D.B.L., O.M., J.S., J.M.A., O.M.S., I.S., W.E.L.), University of Oslo, Norway.
Department of Internal Medicine, Diakonhjemmet Hospital, Oslo, Norway (K.T., E.Ø.).
Circ Res. 2020 Mar 27;126(7):889-906. doi: 10.1161/CIRCRESAHA.119.315641. Epub 2020 Feb 19.
Hypokalemia occurs in up to 20% of hospitalized patients and is associated with increased incidence of ventricular and atrial fibrillation. It is unclear whether these differing types of arrhythmia result from direct and perhaps distinct effects of hypokalemia on cardiomyocytes.
To investigate proarrhythmic mechanisms of hypokalemia in ventricular and atrial myocytes.
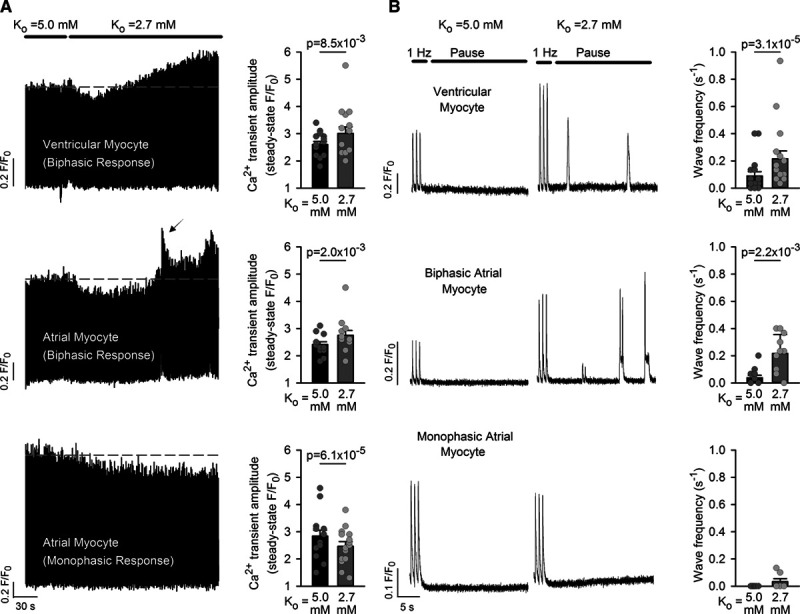
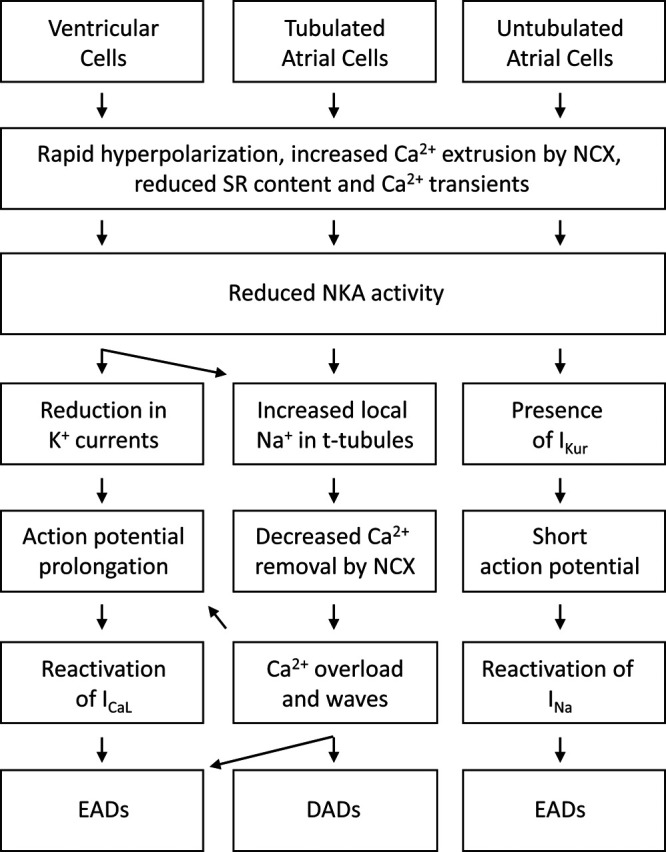
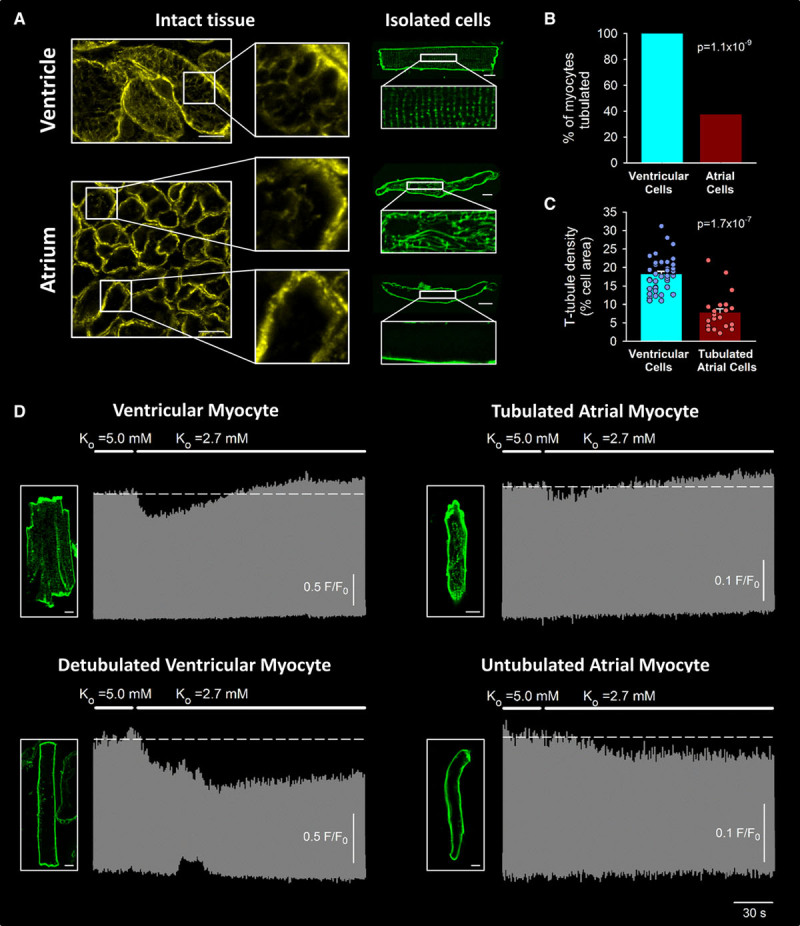
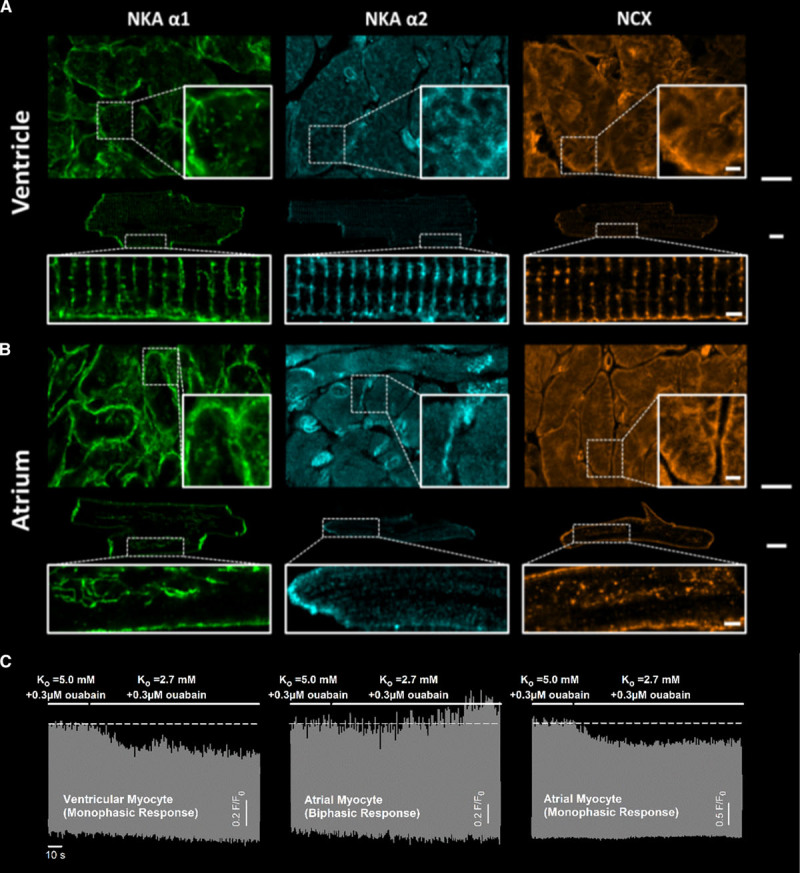
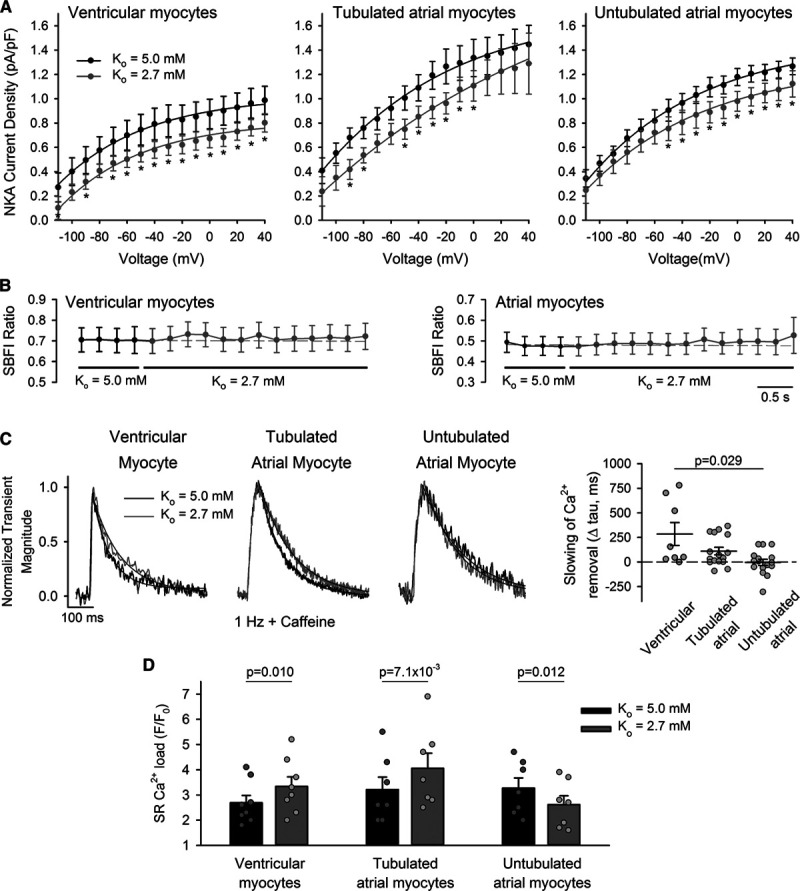
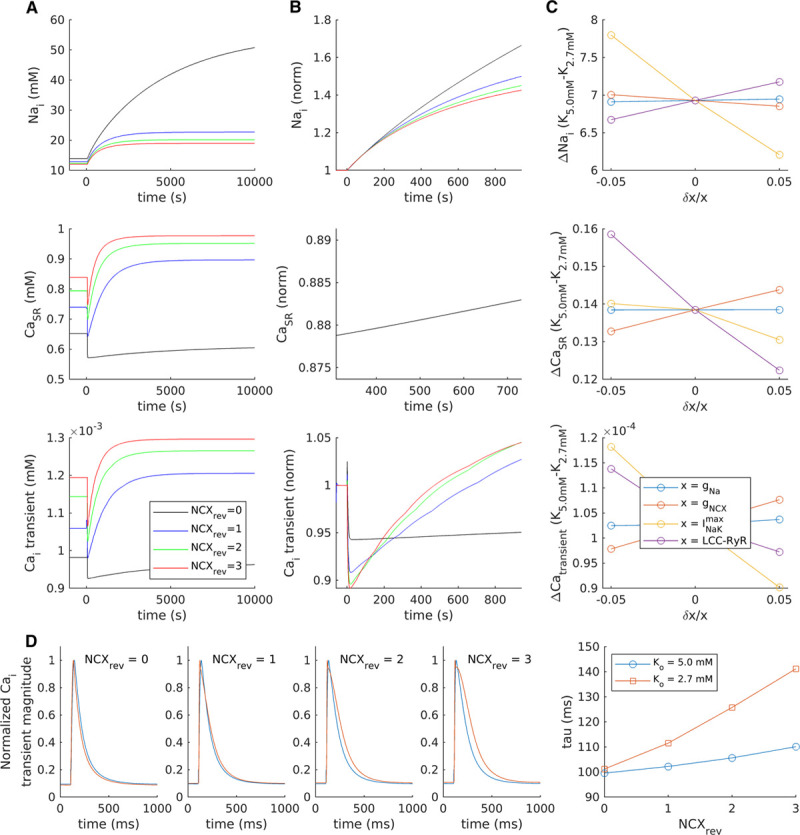
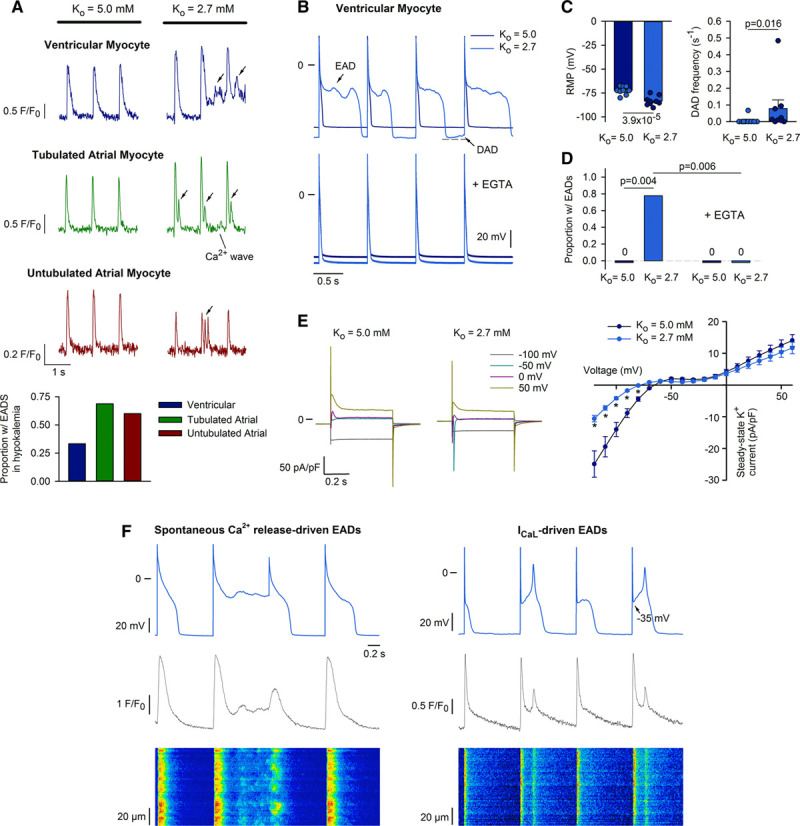
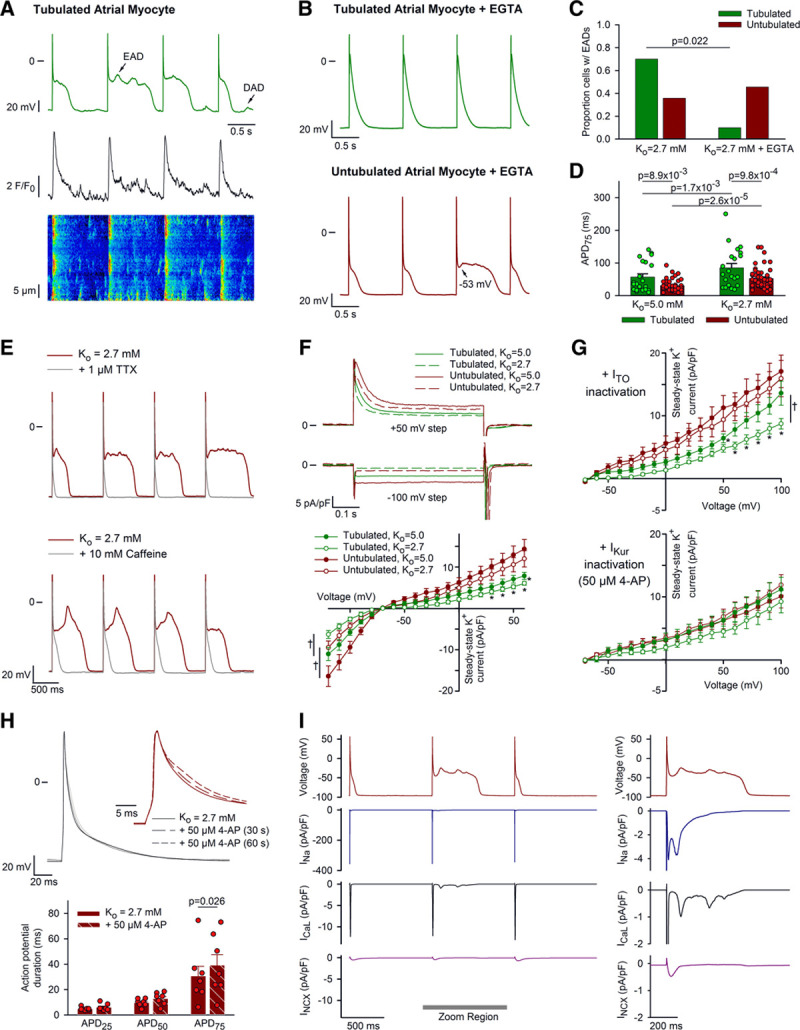
Experiments were performed in isolated rat myocytes exposed to simulated hypokalemia conditions (reduction of extracellular [K] from 5.0 to 2.7 mmol/L) and supported by mathematical modeling studies. Ventricular cells subjected to hypokalemia exhibited Ca overload and increased generation of both spontaneous Ca waves and delayed afterdepolarizations. However, similar Ca-dependent spontaneous activity during hypokalemia was only observed in a minority of atrial cells that were observed to contain t-tubules. This effect was attributed to close functional pairing of the Na-K ATPase and Na-Ca exchanger proteins within these structures, as reduction in Na pump activity locally inhibited Ca extrusion. Ventricular myocytes and tubulated atrial myocytes additionally exhibited early afterdepolarizations during hypokalemia, associated with Ca overload. However, early afterdepolarizations also occurred in untubulated atrial cells, despite Ca quiescence. These phase-3 early afterdepolarizations were rather linked to reactivation of nonequilibrium Na current, as they were rapidly blocked by tetrodotoxin. Na current-driven early afterdepolarizations in untubulated atrial cells were enabled by membrane hyperpolarization during hypokalemia and short action potential configurations. Brief action potentials were in turn maintained by ultra-rapid K current (I); a current which was found to be absent in tubulated atrial myocytes and ventricular myocytes.
Distinct mechanisms underlie hypokalemia-induced arrhythmia in the ventricle and atrium but also vary between atrial myocytes depending on subcellular structure and electrophysiology.
低血钾症可发生于多达 20%的住院患者中,与室性和房性颤动的发生率增加有关。目前尚不清楚这些不同类型的心律失常是否是由低血钾症对心肌细胞的直接影响所致,且这种影响可能具有独特性。
研究低血钾症诱发室性和房性心律失常的机制。
在模拟低血钾条件(将细胞外液[K+]从 5.0 降至 2.7 mmol/L)下,对分离的大鼠心肌细胞进行实验,并结合数学模型研究。低钾时,心室细胞表现为 Ca 超载,自发性 Ca 波和延迟后除极的产生增加。然而,在含有 T 小管的少数心房细胞中仅观察到类似的低钾时 Ca 依赖性自发性活动。这种效应归因于这些结构中 Na-K ATP 酶和 Na-Ca 交换蛋白的紧密功能偶联,因为 Na 泵活性的降低局部抑制了 Ca 外排。此外,低钾时心室肌细胞和具 T 小管的心房肌细胞还表现出早期后除极,伴有 Ca 超载。然而,尽管 Ca 处于静止状态,无 T 小管的心房细胞也会发生早期后除极。这些 3 相早期后除极与非平衡 Na 电流的再激活有关,因为它们很快被河豚毒素阻断。无 T 小管的心房细胞中的 Na 电流驱动的早期后除极是由低钾时的膜超极化和短动作电位构型所引发的。短暂的动作电位继而由超快速 K 电流(I)维持;而在具 T 小管的心房肌细胞和心室肌细胞中则不存在该电流。
心室和心房的低钾血症诱发心律失常的机制不同,而且在心房肌细胞之间也有所不同,这取决于亚细胞结构和电生理学特性。