Meller Menachem M, Goodman Stuart, Gonzalez Mark H, Lau Edmund
Main Line Health, Section of orthopedic surgery, Merion Station, PA (Dr. Meller); the Stanford University Medical Center, Department of Orthopedic Surgery and Bioengineering, Redwood City, CA (Dr. Goodman), the University of Illinois, Department of Orthopedic Surgery, Chicago, Il,(Dr. Gonzalez), Exponent Inc, Health Sciences, Menlo Park, Ca (Mr. Lau).
J Am Acad Orthop Surg Glob Res Rev. 2019 Dec 24;3(12). doi: 10.5435/JAAOSGlobal-D-19-00102. eCollection 2019 Dec.
Patients with morbid obesity, defined as body mass index of greater than 40 kg/m, are being referred for weight loss and bariatric surgery before being accepted for a total knee arthroplasty (TKA). Previous studies have identified the risks associated with doing a TKA in an individual with an increased body mass index. We now present data identifying the same risks in individuals who have undergone bariatric surgery before submitting to TKA.
QUESTIONS/PURPOSES: (1) Has the bariatric surgery improved the risk profile for the subsequent TKA? (2) Does the type of bariatric procedure matter?
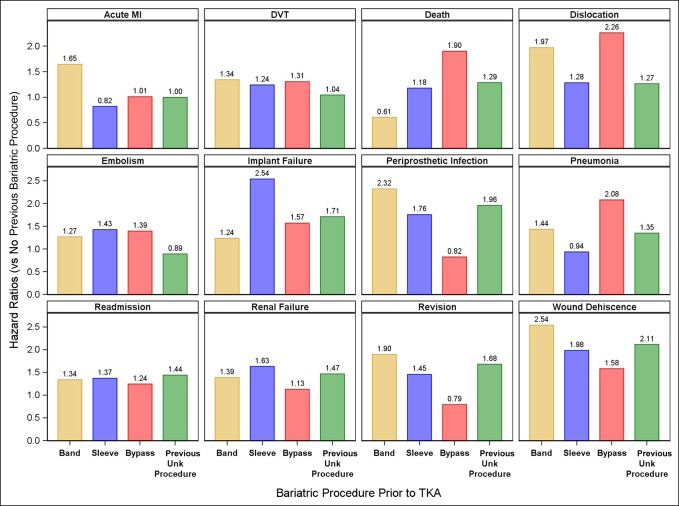
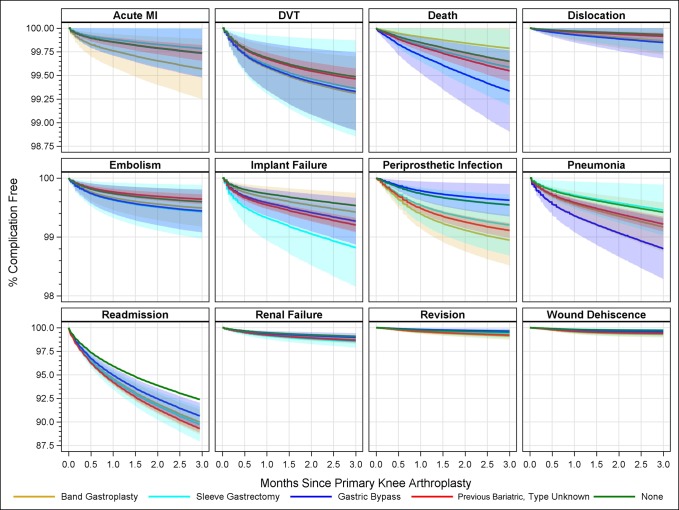
A retrospective cohort study was conducted of patients who underwent bariatric surgery followed by TKA using Medicare hospital claims data. A study was undertaken using the Current Procedure Terminology codes and and for bariatric surgery. These identified entries were then cross-referenced to individuals who later underwent TKA, identified by CPT 27447, between 2004 and 2016. Twelve different types of complications which occurred in the 90-day period after the TKA were analyzed.
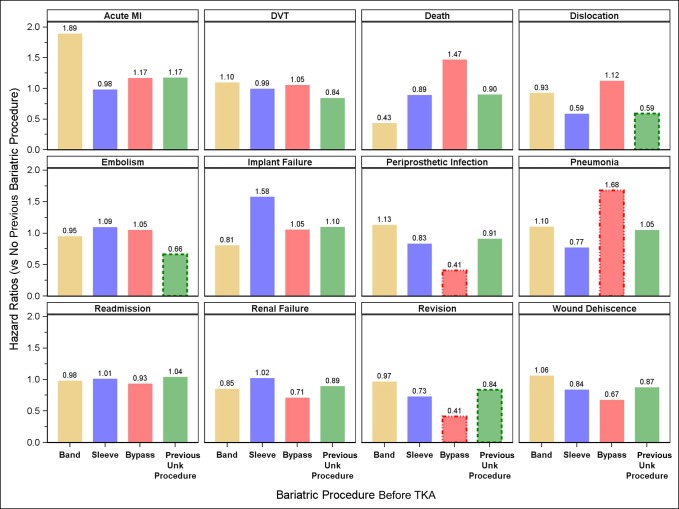
Postbariatric bypass surgery patients showed a markedly elevated risk in most complications examined. In each category, the type of previous gastric surgery had notable differences in the post-TKA complication profile. In the implant failure category, the data demonstrated an even greater risk after a gastric bypass. When postbariatric patients were compared with morbidly obese individuals who had not undergone bariatric surgery, the hazard ratios (HRs) were markedly elevated for death (HR 1.47/bypass), implant failure (HR 1.58/sleeve), and pneumonia (HR 1.68/bypass).
(1) Submitting to bariatric surgery is not sufficient to normalize risks. (2) The type of previous bariatric procedure is associated with the type of complications encountered. (3) We were unable to attribute TKA to bariatric failures. (4) Health systems and health care providers should be cautious in withholding care for patients with morbid obesity.
病态肥胖患者(定义为体重指数大于40kg/m²)在接受全膝关节置换术(TKA)之前,会被转介进行减重和减肥手术。先前的研究已经确定了在体重指数增加的个体中进行TKA的相关风险。我们现在展示的数据表明,在接受TKA之前接受过减肥手术的个体中也存在同样的风险。
问题/目的:(1)减肥手术是否改善了后续TKA的风险状况?(2)减肥手术的类型重要吗?
使用医疗保险医院理赔数据,对接受减肥手术随后进行TKA的患者进行了一项回顾性队列研究。使用当前手术操作术语代码进行减肥手术研究。然后将这些识别出的条目与后来接受TKA的个体进行交叉参考,这些个体通过CPT 27447在2004年至2016年间被识别。分析了TKA后90天内发生的12种不同类型的并发症。
减肥旁路手术后的患者在大多数检查的并发症中显示出明显升高的风险。在每个类别中,先前胃手术的类型在TKA后并发症情况方面有显著差异。在植入物失败类别中,数据显示胃旁路手术后风险更高。当将减肥手术后的患者与未接受减肥手术的病态肥胖个体进行比较时,死亡(风险比1.47/旁路)、植入物失败(风险比1.58/袖状胃切除术)和肺炎(风险比1.68/旁路)的风险比显著升高。
(1)接受减肥手术不足以使风险正常化。(2)先前减肥手术的类型与所遇到的并发症类型相关。(3)我们无法将TKA归因于减肥手术失败。(4)卫生系统和医疗保健提供者在拒绝为病态肥胖患者提供治疗时应谨慎。