Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
Brigham and Women's Hospital, Harvard University, Boston, MA, USA.
J Natl Cancer Inst. 2020 Dec 14;112(12):1266-1274. doi: 10.1093/jnci/djaa028.
The National Cancer Institute Moonshot research initiative calls for improvements in the analysis and reporting of treatment toxicity to advise key stakeholders on treatment tolerability and inform regulatory and clinical decision making. This study illustrates alternative approaches to toxicity evaluation using the National Surgical Adjuvant Breast and Bowel Project R-04 clinical trial as an example.
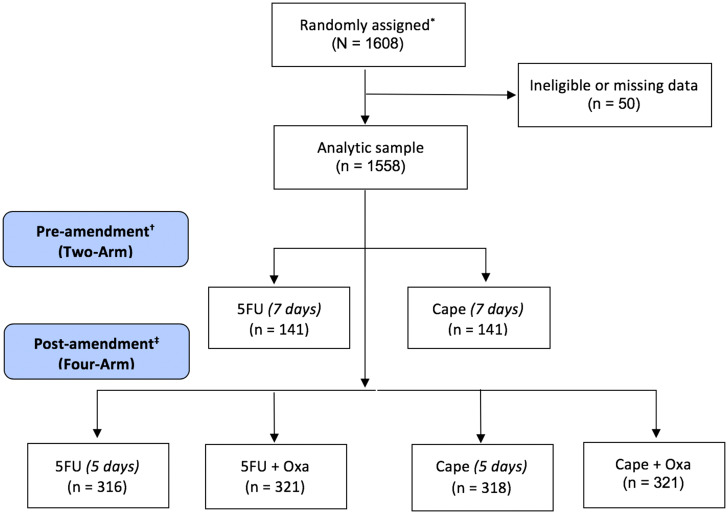
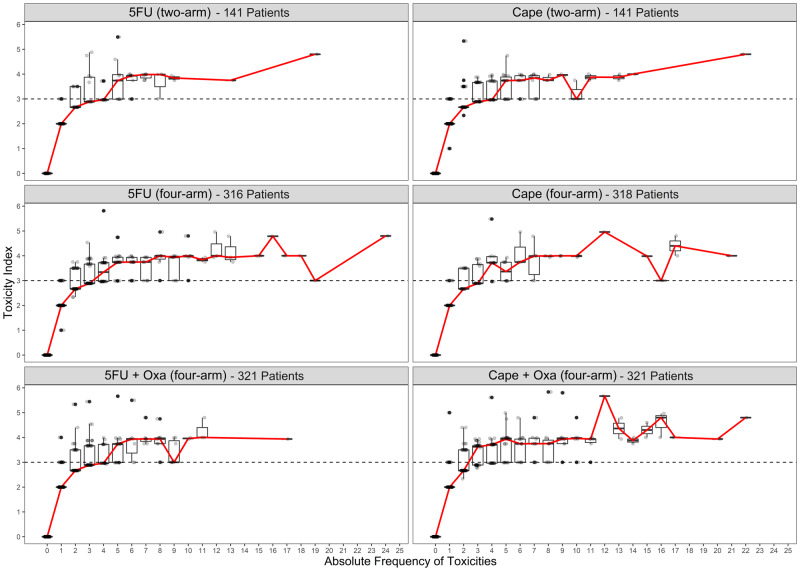
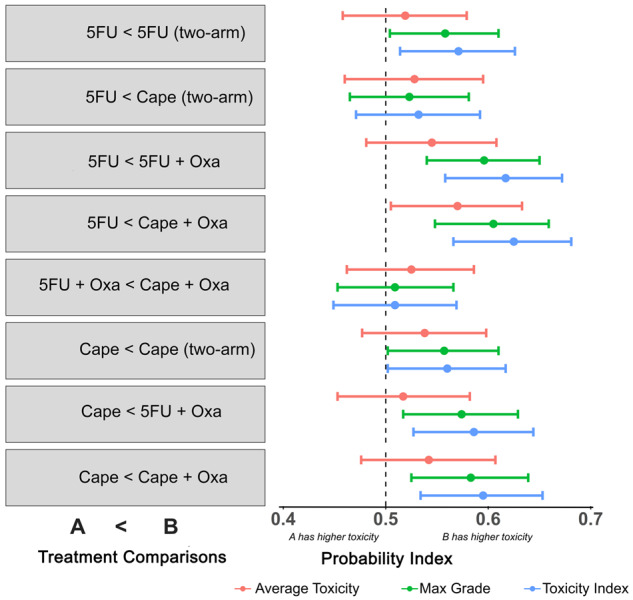
National Surgical Adjuvant Breast and Bowel Project R-04 was a neoadjuvant chemoradiation trial in stage II-III rectal cancer patients. A 2 x 2 factorial design was used to evaluate whether the addition of oxaliplatin (Oxa) to 5-fluorouracil (5FU) or capecitabine (Cape) with radiation therapy improved local-regional tumor control. The toxicity index (TI), which accounts for the frequency and severity of toxicities, was compared across treatments using multivariable probabilistic index models, where Pr A < B indicates the probability that higher values of TI were observed for A when compared with B. Baseline age, sex, performance status, body mass index, surgery type, and stage were evaluated as independent risk factors.
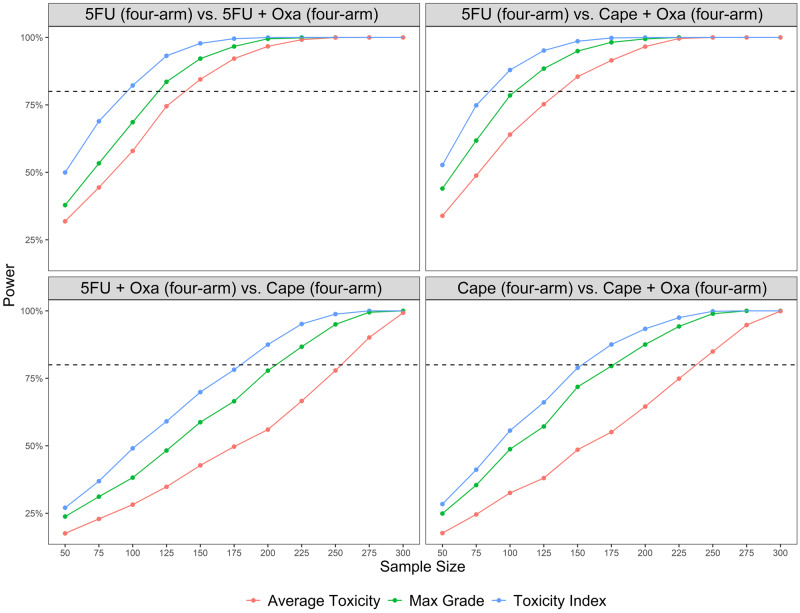
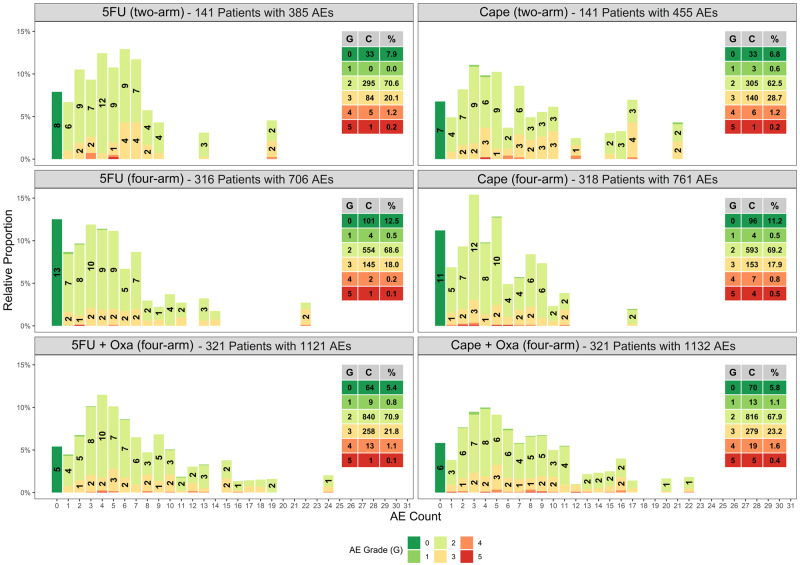
A total of 4560 toxicities from 1558 patients were analyzed. Results from adjusted probabilistic index models indicate that oxaliplatin-containing regimens had statistically significant (P < .001) probability (Pr) for higher TI compared with regimens without oxaliplatin (Pr 5FU < 5FU + Oxa = 0.619, 95% confidence interval [CI] = 0.560 to 0.674; Pr 5FU < Cape + Oxa = 0.627, 95% CI = 0.568 to 0.682; Pr Cape < 5FU + Oxa = 0.587, 95% 0.527 to 0.644; and Pr Cape < Cape + Oxa = 0.596, 95% 0.536 to 0.653). When compared with other existing toxicity analysis methods, TI provided greater power to detect differences between treatments.
This article uses standard data collected in a cancer clinical trial to introduce descriptive and analytic methods that account for the additional burden of multiple toxicities. These methods may provide a more accurate description of a patient's treatment experience that could lead to individualized dosing for better toxicity control. Future research will evaluate the generalizability of these findings in trials with similar drugs.
美国国家癌症研究所的“登月”研究计划呼吁改进治疗毒性的分析和报告,以便就治疗耐受性向主要利益相关者提供建议,并为监管和临床决策提供信息。本研究以国家外科辅助乳腺和肠道项目 R-04 临床试验为例,说明了使用替代方法评估毒性的方法。
国家外科辅助乳腺和肠道项目 R-04 是一项 II-III 期直肠癌患者的新辅助放化疗试验。采用 2x2 析因设计来评估奥沙利铂(Oxa)联合氟尿嘧啶(5FU)或卡培他滨(Cape)与放疗是否能提高局部区域肿瘤控制率。毒性指数(TI)考虑了毒性的频率和严重程度,使用多变量概率指数模型对不同治疗方法进行比较,其中 Pr A < B 表示与 B 相比,观察到 TI 值较高的 A 的概率。基线年龄、性别、表现状态、体重指数、手术类型和分期被评估为独立风险因素。
对 1558 名患者的 4560 种毒性进行了分析。调整后的概率指数模型结果表明,含奥沙利铂的方案与不含奥沙利铂的方案相比,TI 值具有统计学显著差异(P < 0.001)(Pr 5FU < 5FU + Oxa = 0.619,95%置信区间 [CI] = 0.560 至 0.674;Pr 5FU < Cape + Oxa = 0.627,95% CI = 0.568 至 0.682;Pr Cape < 5FU + Oxa = 0.587,95% CI = 0.527 至 0.644;Pr Cape < Cape + Oxa = 0.596,95% CI = 0.536 至 0.653)。与其他现有的毒性分析方法相比,TI 提供了更大的能力来检测治疗方法之间的差异。
本文使用癌症临床试验中收集的标准数据,介绍了考虑多种毒性额外负担的描述性和分析方法。这些方法可能更准确地描述患者的治疗体验,从而实现个体化剂量以更好地控制毒性。未来的研究将评估这些发现在具有类似药物的试验中的普遍性。