Buonauro Agostino, Santoro Ciro, Galderisi Maurizio, Canora Angelo, Sorrentino Regina, Esposito Roberta, Lembo Maria, Canonico Mario Enrico, Ilardi Federica, Fazio Valeria, Golia Bruno, Sanduzzi Alessandro, Bocchino Marialuisa
Department of Advanced Biomedical Sciences, Federico II University Hospital, 80131 Naples, Italy.
Department of Clinical Medicine and Surgery, Federico II University, Monaldi Hospital, 80131 Naples, Italy.
J Clin Med. 2020 Feb 21;9(2):587. doi: 10.3390/jcm9020587.
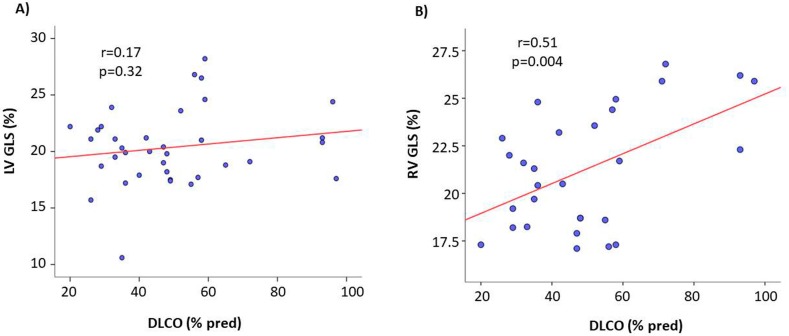
Left ventricular (LV) and right ventricular (RV) dysfunction is recognized in idiopathic pulmonary fibrosis (IPF). Little is known about cardiac involvement in non-idiopathic pulmonary fibrosis (no-IPF). This issue can be explored by advanced echocardiography. Thirty-three clinically stable and therapy-naive fibrotic IPF and 28 no-IPF patients, and 30 healthy controls were enrolled. Exclusion criteria were autoimmune systemic diseases, coronary disease, heart failure, primary cardiomyopathies, chronic obstructive lung diseases, pulmonary embolism, primary pulmonary hypertension. Lung damage was evaluated by diffusion capacity for carbon monoxide (DLCO). All participants underwent an echo-Doppler exam including 2D global longitudinal strain (GLS) of both ventricles and 3D echocardiographic RV ejection fraction (RVEF). We observed LV diastolic dysfunction in IPF and no-IPF, and LV GLS but not LV EF reduction only in IPF. RV diastolic and RV GLS abnormalities were observed in IPF versus both controls and no-IPF. RV EF did not differ significantly between IPF and no-IPF. DLCO and RV GLS were associated in the pooled pulmonary fibrosis population and in the IPF subgroup (β = 0.708, < 0.001), independently of confounders including pulmonary arterial systolic pressure. Our data highlight the unique diagnostic capabilities of GLS in distinguishing early cardiac damage of IPF from no-IPF patients.
特发性肺纤维化(IPF)患者存在左心室(LV)和右心室(RV)功能障碍。对于非特发性肺纤维化(no - IPF)患者的心脏受累情况知之甚少。这一问题可通过先进的超声心动图进行探究。研究纳入了33例临床稳定且未接受过治疗的纤维化IPF患者、28例no - IPF患者以及30名健康对照者。排除标准包括自身免疫性系统性疾病、冠状动脉疾病、心力衰竭、原发性心肌病、慢性阻塞性肺疾病、肺栓塞、原发性肺动脉高压。通过一氧化碳弥散量(DLCO)评估肺损伤情况。所有参与者均接受了超声多普勒检查,包括双心室的二维整体纵向应变(GLS)和三维超声心动图右心室射血分数(RVEF)。我们观察到IPF和no - IPF患者均存在左心室舒张功能障碍,且仅IPF患者存在左心室GLS降低而非左心室射血分数(EF)降低。与对照组和no - IPF患者相比,IPF患者存在右心室舒张和右心室GLS异常。IPF和no - IPF患者之间的右心室EF无显著差异。在合并的肺纤维化人群和IPF亚组中,DLCO与右心室GLS相关(β = 0.708,< 0.001),且独立于包括肺动脉收缩压在内的混杂因素。我们的数据突出了GLS在区分IPF患者与no - IPF患者早期心脏损伤方面的独特诊断能力。