Centre for Cardiovascular Science, University of Edinburgh, Edinburgh, United Kingdom.
Aetion Inc, New York, New York.
JAMA Netw Open. 2020 Feb 5;3(2):e200107. doi: 10.1001/jamanetworkopen.2020.0107.
Patients with nonvalvular atrial fibrillation at risk of stroke should receive oral anticoagulants (OAC). However, approximately 1 in 8 patients in the Global Anticoagulant Registry in the Field (GARFIELD-AF) registry are treated with antiplatelet (AP) drugs in addition to OAC, with or without documented vascular disease or other indications for AP therapy.
To investigate baseline characteristics and outcomes of patients who were prescribed OAC plus AP therapy vs OAC alone.
DESIGN, SETTING, AND PARTICIPANTS: Prospective cohort study of the GARFIELD-AF registry, an international, multicenter, observational study of adults aged 18 years and older with recently diagnosed nonvalvular atrial fibrillation and at least 1 risk factor for stroke enrolled between March 2010 and August 2016. Data were extracted for analysis in October 2017 and analyzed from April 2018 to June 2019.
Participants received either OAC plus AP or OAC alone.
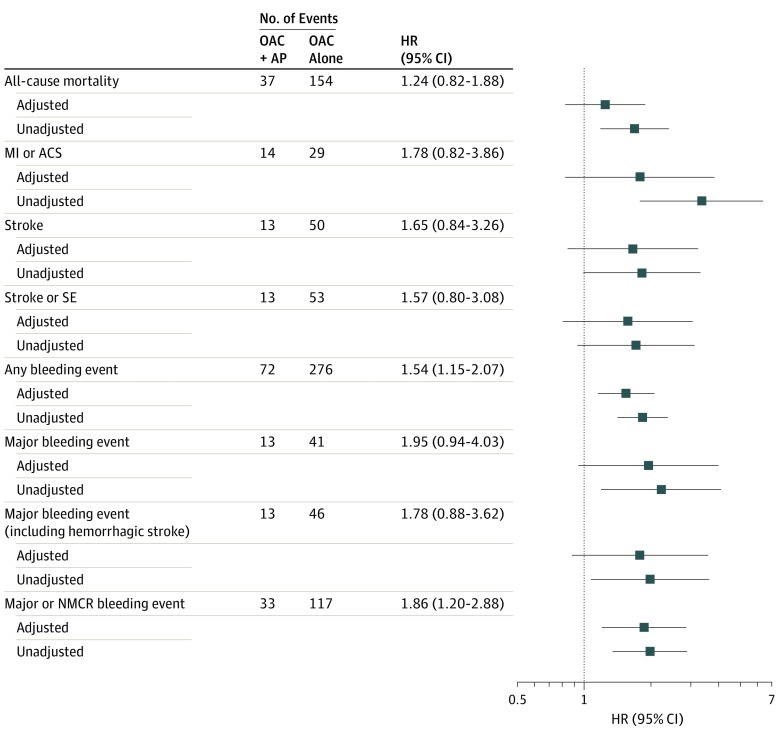
Clinical outcomes were measured over 3 and 12 months. Outcomes were adjusted for 40 covariates, including baseline conditions and medications.
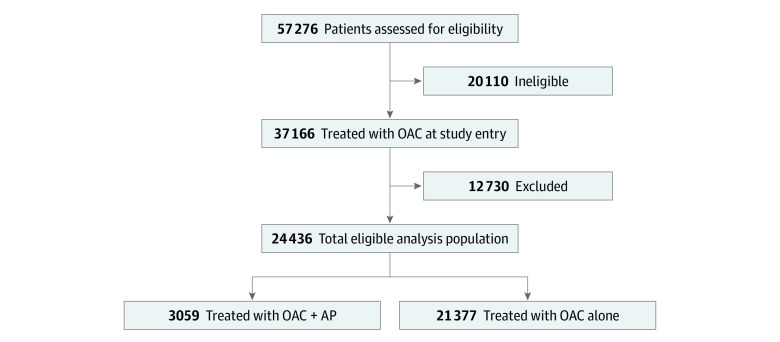
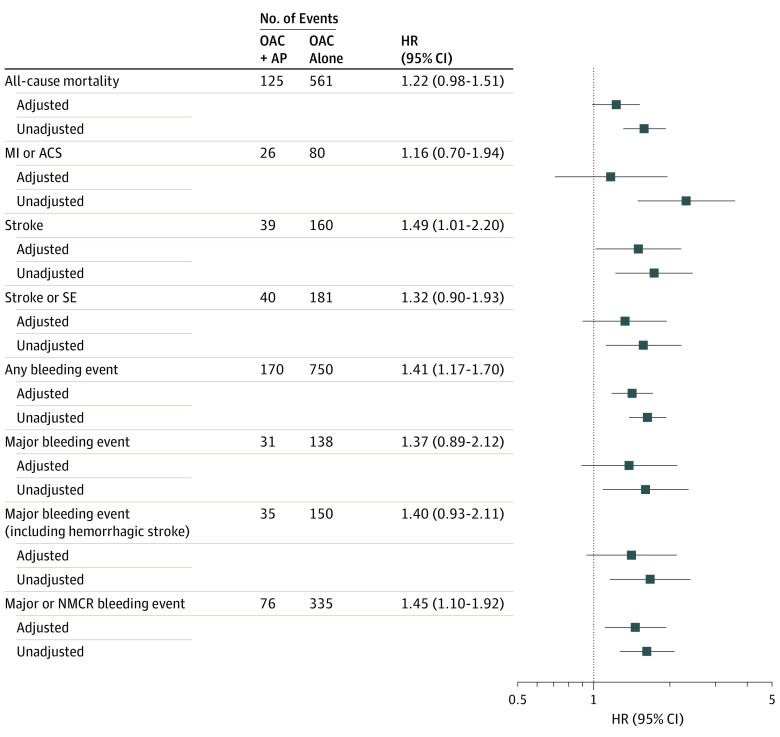
A total of 24 436 patients (13 438 [55.0%] male; median [interquartile range] age, 71 [64-78] years) were analyzed. Among eligible patients, those receiving OAC plus AP therapy had a greater prevalence of cardiovascular indications for AP, including acute coronary syndromes (22.0% vs 4.3%), coronary artery disease (39.1% vs 9.8%), and carotid occlusive disease (4.8% vs 2.0%). Over 1 year, patients treated with OAC plus AP had significantly higher incidence rates of stroke (adjusted hazard ratio [aHR], 1.49; 95% CI, 1.01-2.20) and any bleeding event (aHR, 1.41; 95% CI, 1.17-1.70) than those treated with OAC alone. These patients did not show evidence of reduced all-cause mortality (aHR, 1.22; 95% CI, 0.98-1.51). Risk of acute coronary syndrome was not reduced in patients taking OAC plus AP compared with OAC alone (aHR, 1.16; 95% CI, 0.70-1.94). Patients treated with OAC plus AP also had higher rates of all clinical outcomes than those treated with OAC alone over the short term (3 months).
This study challenges the practice of coprescribing OAC plus AP unless there is a clear indication for adding AP to OAC therapy in newly diagnosed atrial fibrillation.
有卒中风险的非瓣膜性心房颤动患者应接受口服抗凝剂(OAC)治疗。然而,GARFIELD-AF 注册研究中约有 1/8 的患者除 OAC 外还同时接受抗血小板(AP)药物治疗,无论是否存在血管疾病或其他 AP 治疗适应证。
旨在研究同时接受 OAC 和 AP 治疗与单独接受 OAC 治疗的患者的基线特征和结局。
设计、地点和参与者:这是一项对 GARFIELD-AF 注册研究的前瞻性队列研究,该研究为国际性、多中心、观察性研究,纳入了 2010 年 3 月至 2016 年 8 月间年龄在 18 岁及以上、新近诊断为非瓣膜性心房颤动且至少存在 1 项卒中风险因素的患者。2017 年 10 月提取数据进行分析,并于 2018 年 4 月至 2019 年 6 月进行分析。
患者接受 OAC 加 AP 或 OAC 单独治疗。
在 3 个月和 12 个月时测量临床结局。结局经 40 项协变量进行调整,包括基线状况和药物。
共纳入 24436 例患者(13438 例[55.0%]为男性;中位[四分位间距]年龄为 71[64-78]岁)。在合格患者中,接受 OAC 加 AP 治疗的患者有更多的 AP 心血管适应证,包括急性冠状动脉综合征(22.0%比 4.3%)、冠心病(39.1%比 9.8%)和颈动脉闭塞性疾病(4.8%比 2.0%)。在 1 年期间,与单独接受 OAC 治疗的患者相比,接受 OAC 加 AP 治疗的患者卒中(调整后的危险比[HR],1.49;95%CI,1.01-2.20)和任何出血事件(调整后的 HR,1.41;95%CI,1.17-1.70)发生率显著更高。这些患者并未表现出全因死亡率降低的证据(调整后的 HR,1.22;95%CI,0.98-1.51)。与单独接受 OAC 治疗相比,接受 OAC 加 AP 治疗的患者发生急性冠状动脉综合征的风险并未降低(调整后的 HR,1.16;95%CI,0.70-1.94)。与单独接受 OAC 治疗的患者相比,接受 OAC 加 AP 治疗的患者在短期(3 个月)内也具有更高的所有临床结局发生率。
这项研究对在新发心房颤动中除 OAC 外同时加用 AP 的做法提出了质疑,除非有明确的指征需要将 AP 加至 OAC 治疗中。