Liu Ruiquan, Deng Zhu, Zhang Li, Liu Yin, Wang Zheng, Yu Yanbing
Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, People's Republic of China.
Department of Neurosurgery, China-Japan Friendship Hospital, Beijing, People's Republic of China.
J Pain Res. 2020 Feb 5;13:301-312. doi: 10.2147/JPR.S225188. eCollection 2020.
Microvascular decompression (MVD) and MVD combined with partial sensory rhizotomy (PSR) are effective surgical treatments for idiopathic trigeminal neuralgia (TN). The aim of this study was to compare the long-term outcomes of both MVD and MVD+PSR for the treatment of TN and to identify the factors that may influence the long-term outcomes after MVD or MVD+PSR.
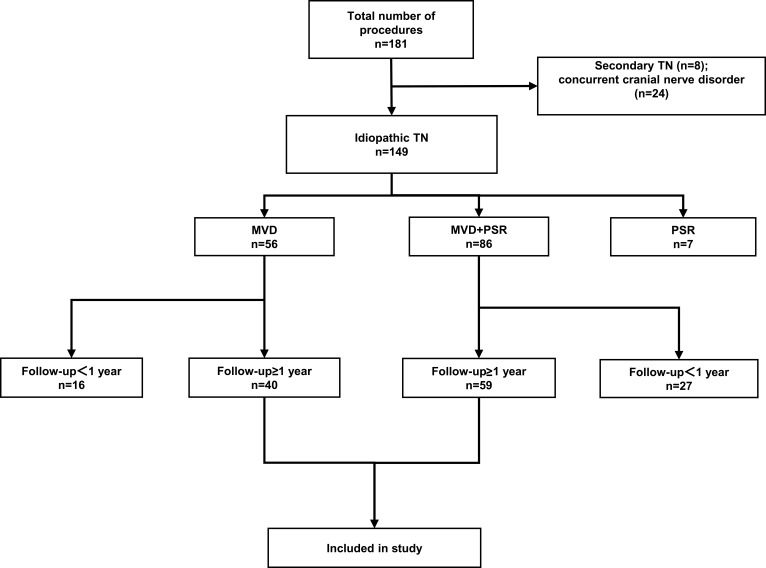
From March 2009 to December 2017, 99 patients with idiopathic TN who underwent MVD or MVD+PSR in our hospital (40 MVD, 59 MVD+PSR) were included in the study. The indications for MVD+PSR were as follows: vessels only contacted the nerve root, absence of arterial conflict, or failing to completely decompress from the arteries or veins. All patients were treated by one neurosurgeon and were followed up for at least 1 year. The outcomes were assessed with the Barrow Neurological Institute (BNI) Pain Intensity Scale.
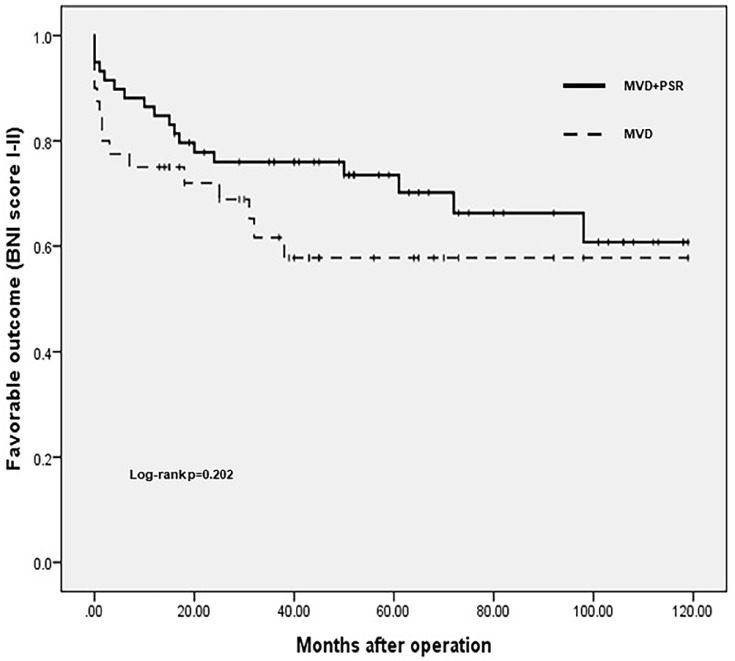
The average follow-up duration was 63.0 months (range, 13.2-118.8 months). Patients in the MVD group were younger than those in the MVD+PSR group (55.1 years and 60.5 years, respectively, P=0.012). A total of 62.5% of the patients in the MVD group and 69.5% of the patients in the MVD+PSR group had favorable long-term outcomes. The Kaplan-Meier survival analysis showed no significant difference in long-term outcomes between the two groups (P=0.202). No factors were associated with long-term outcomes after MVD. For MVD+PSR, a long duration of the disease (odds ratio (OR) 6.967, P=0.016) was associated with unfavorable long-term outcomes, whereas pure arterial compression (OR 0.131, P=0.013) was associated with favorable long-term outcomes.
For patients who are not suitable to undergo pure MVD, MVD+PSR can be used as an effective alternative. For MVD+PSR, patients with a long duration of symptoms may have poor long-term outcomes, while patients with pure arterial compression may have favorable long-term outcomes.
微血管减压术(MVD)以及MVD联合部分感觉神经根切断术(PSR)是治疗特发性三叉神经痛(TN)的有效外科手术方法。本研究旨在比较MVD和MVD+PSR治疗TN的长期疗效,并确定可能影响MVD或MVD+PSR术后长期疗效的因素。
2009年3月至2017年12月期间,我院99例行MVD或MVD+PSR的特发性TN患者纳入本研究(40例行MVD,59例行MVD+PSR)。MVD+PSR的适应证如下:血管仅接触神经根、无动脉冲突或未能从动脉或静脉完全减压。所有患者均由一名神经外科医生治疗,并随访至少1年。采用巴罗神经学研究所(BNI)疼痛强度量表评估疗效。
平均随访时间为63.0个月(范围13.2 - 118.8个月)。MVD组患者比MVD+PSR组患者年轻(分别为55.1岁和60.5岁,P = 0.012)。MVD组62.5%的患者和MVD+PSR组69.5%的患者有良好的长期疗效。Kaplan-Meier生存分析显示两组长期疗效无显著差异(P = 0.202)。MVD术后无因素与长期疗效相关。对于MVD+PSR,病程长(比值比(OR)6.967,P = 0.016)与不良长期疗效相关,而单纯动脉压迫(OR 0.131,P = 0.013)与良好长期疗效相关。
对于不适合单纯行MVD的患者,MVD+PSR可作为一种有效的替代方法。对于MVD+PSR,症状持续时间长的患者长期疗效可能较差,而单纯动脉压迫的患者长期疗效可能较好。