Derebail Vimal K, Rheault Michelle N, Kerlin Bryce A
UNC Kidney Center, Division of Nephrology and Hypertension, Department of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA.
Department of Pediatrics, Division of Pediatric Nephrology, University of Minnesota Masonic Children's Hospital, Minneapolis, Minnesota, USA.
Kidney Int. 2020 Apr;97(4):664-675. doi: 10.1016/j.kint.2019.11.027. Epub 2019 Dec 24.
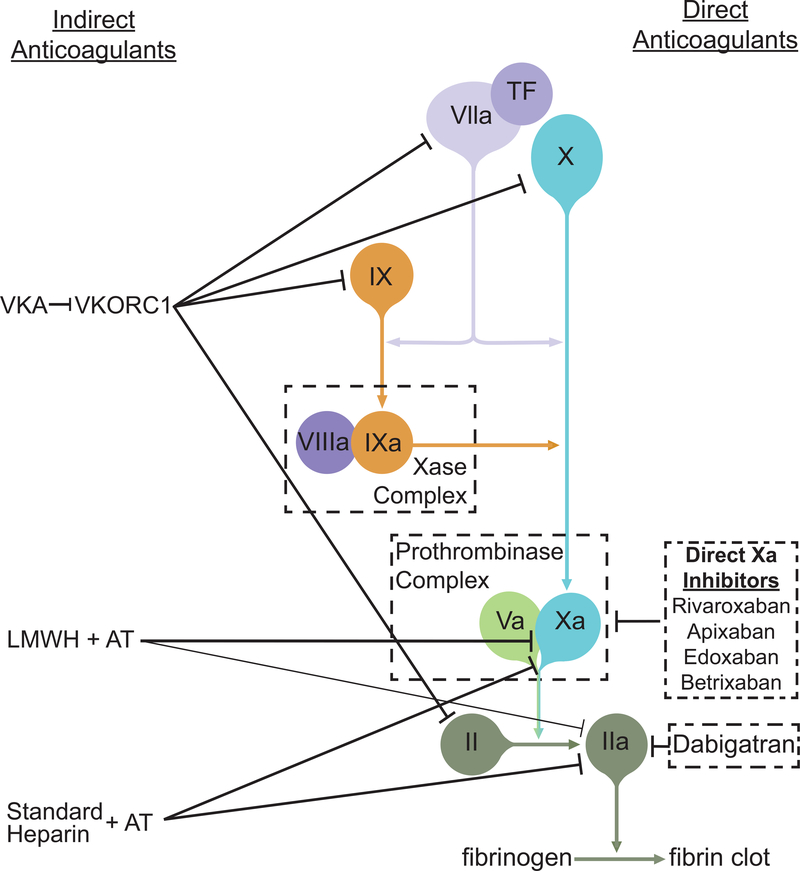
The anticoagulation field is experiencing a renaissance that began with regulatory approval of the direct thrombin inhibitor dabigatran, a direct oral anticoagulant (DOAC), in 2010. The DOAC medication class has rapidly evolved to include the additional approval of 4 direct factor Xa inhibitors. Commensurately, DOAC use has increased and collectively account for the majority of new anticoagulant prescriptions. Despite exclusion of patients with moderate-to-severe kidney disease from most pivotal DOAC trials, DOACs are increasingly used in this setting. An advantage of DOACs is similar or improved antithrombotic efficacy with less bleeding risk when compared with traditional agents. Several post hoc analyses, retrospective studies, claims data studies, and meta-analyses suggest that these benefits extend to patients with kidney disease. However, the lack of randomized controlled trial data in specific kidney disease settings, with their unique pathophysiology, should be a call to action for the kidney community to systematically study these agents, especially because early data suggest that DOACs may pose less risk of anticoagulant-related nephropathy than do vitamin K antagonists. Most DOACs are renally cleared and are significantly protein bound in circulation; thus, the pharmacokinetics of these drugs are influenced by reduced renal function and proteinuria. DOACs are susceptible to altered metabolism by P-glycoprotein inhibitors and inducers, including drugs commonly used for the management of kidney disease comorbidities. We summarize the currently available literature on DOAC use in kidney disease and illustrate knowledge gaps that represent important opportunities for prospective investigation.
抗凝领域正在经历一场复兴,这场复兴始于2010年直接凝血酶抑制剂达比加群(一种直接口服抗凝剂,DOAC)获得监管批准。DOAC药物类别迅速发展,又有4种直接因子Xa抑制剂获得批准。相应地,DOAC的使用有所增加,共同占据了大多数新的抗凝处方。尽管大多数关键的DOAC试验排除了中重度肾病患者,但DOAC在这种情况下的使用越来越多。与传统药物相比,DOAC的一个优点是具有相似或更好的抗血栓疗效,同时出血风险更低。多项事后分析、回顾性研究、索赔数据研究和荟萃分析表明,这些益处也适用于肾病患者。然而,在具有独特病理生理学的特定肾病环境中缺乏随机对照试验数据,这应该促使肾脏学界采取行动,系统地研究这些药物,特别是因为早期数据表明,DOAC可能比维生素K拮抗剂引起抗凝相关肾病的风险更低。大多数DOAC通过肾脏清除,在循环中与蛋白质有显著结合;因此,这些药物的药代动力学受肾功能减退和蛋白尿的影响。DOAC易受P-糖蛋白抑制剂和诱导剂影响而发生代谢改变,这些抑制剂和诱导剂包括常用于治疗肾病合并症的药物。我们总结了目前关于DOAC在肾病中应用的文献,并阐述了知识空白,这些空白代表了前瞻性研究的重要机会。