Department for Orthopaedic and Trauma Surgery, University Medicine Carl Gustav Carus, Fetscherstr. 74, 01307, Dresden, Germany.
Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1169-1176. doi: 10.1007/s00167-019-05843-2. Epub 2020 Feb 28.
Pain management after total knee arthroplasty (TKA) is still under debate. Continuous peripheral nerve blocks (PNB) can provide long pain relief but impair muscle function. Continuous intraarticular analgesia could result in longer pain relief than local infiltration analgesia without negative effects on muscle function. This study investigated the efficacy of pain control between PNB's and continuous intraarticular analgesia after TKA.
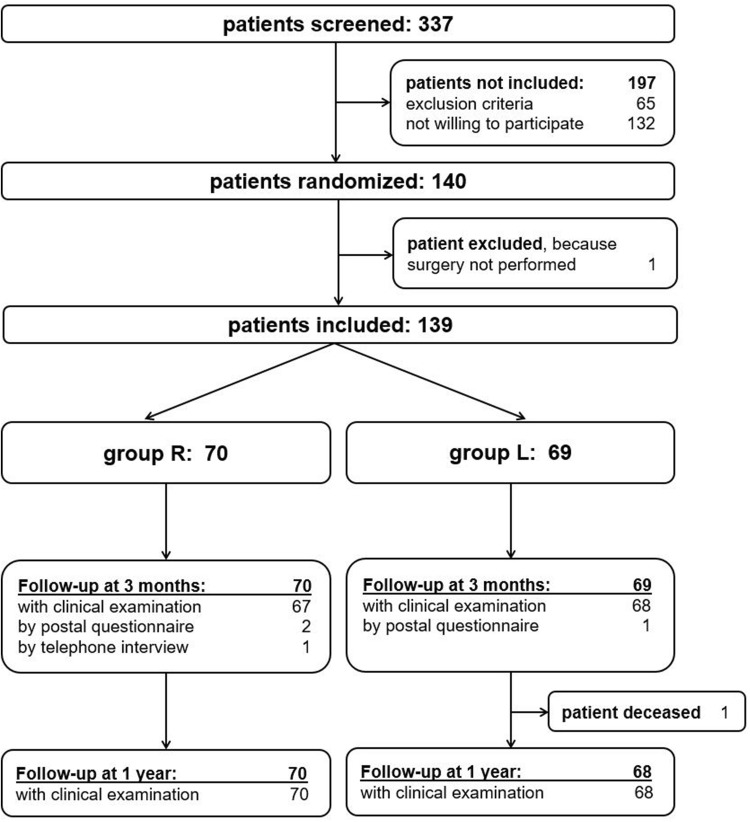
A prospective randomized study on 140 patients undergoing TKA was performed. Patients received either a combination of continuous femoral nerve block, continuous sciatic nerve block and single-shot obturator nerve block (group R) or a local infiltration analgesia and a continuous intraarticular catheter with ropivacaine (group L). Primary outcome was pain measured on a numerical rating scale. Knee function, patient-reported outcome (PRO) and adverse events were assessed until 1 year after surgery.
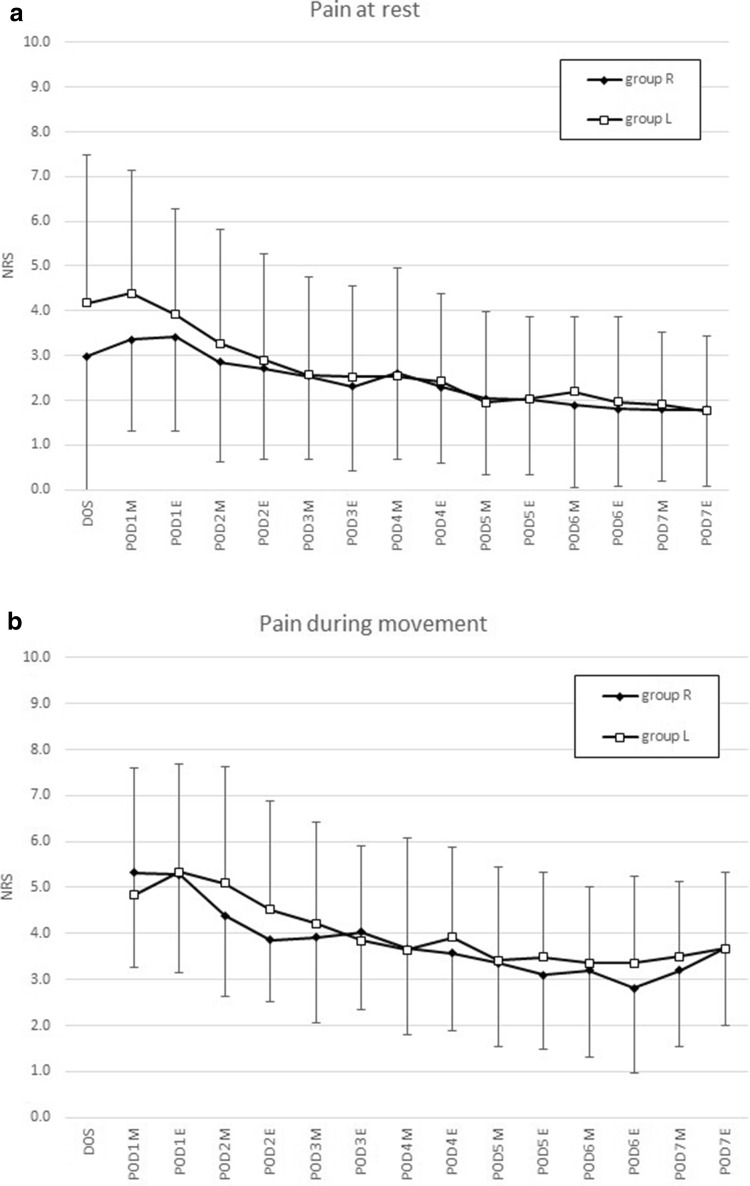
Pain at rest was lower in group R on the day of surgery (mean NRS 3.0 vs. 4.2) and the morning of postoperative day 1 (mean NRS 3.4 vs. 4.4). Motor blockade longer than postoperative day 3 occurred more often in group R compared to group L (15.3% vs. 1.5%). Pain levels, PRO and satisfaction 3-month and 1-year after surgery were similar.
Continuous PNB's were slightly more effective in the first 24 h after surgery but were associated more often with motor blockade which should be avoided. It must be balanced if the small amount of better pain relief immediately after surgery justifies the risks associated with motor blockade following PNB's.
I.
全膝关节置换术(TKA)后疼痛管理仍存在争议。连续外周神经阻滞(PNB)可提供长期疼痛缓解,但会损害肌肉功能。连续关节内镇痛可能比局部浸润性镇痛提供更长时间的疼痛缓解,而不会对肌肉功能产生负面影响。本研究旨在比较 TKA 后 PNB 和连续关节内镇痛的疼痛控制效果。
对 140 例行 TKA 的患者进行前瞻性随机研究。患者接受连续股神经阻滞、连续坐骨神经阻滞和单次闭孔神经阻滞(R 组)或局部浸润性镇痛和连续关节内罗哌卡因导管(L 组)。主要结局是通过数字评分量表测量疼痛。评估膝关节功能、患者报告的结局(PRO)和不良事件,直到术后 1 年。
R 组患者在手术当天(平均 NRS 3.0 比 4.2)和术后第 1 天早晨(平均 NRS 3.4 比 4.4)静息时疼痛较低。与 L 组相比,R 组术后第 3 天以上出现运动阻滞的情况更为常见(15.3%比 1.5%)。术后 3 个月和 1 年时,疼痛水平、PRO 和满意度相似。
连续 PNB 在术后前 24 小时内的效果稍好,但与运动阻滞的相关性更高,应避免这种情况。必须权衡利弊,如果术后立即使用 PNB 能获得少量更好的疼痛缓解,是否值得冒与运动阻滞相关的风险。
I。