van den Dries Carline J, van Doorn Sander, Rutten Frans H, Oudega Ruud, van de Leur Sjef J C M, Elvan Arif, Oude Grave Lisa, Bilo Henk J G, Moons Karel G M, Hoes Arno W, Geersing Geert-Jan
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht/Utrecht University, Str. 6.131, PO Box 85500, 3508 GA Utrecht, the Netherlands.
Thrombosis Service, Isala Hospital Zwolle, Postbus 10400, 8000 GK Zwolle, the Netherlands.
Eur Heart J. 2020 Aug 7;41(30):2836-2844. doi: 10.1093/eurheartj/ehaa055.
To evaluate whether integrated care for atrial fibrillation (AF) can be safely orchestrated in primary care.
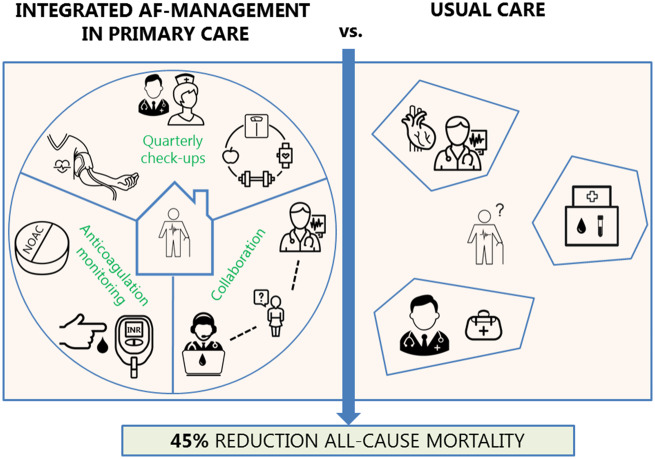
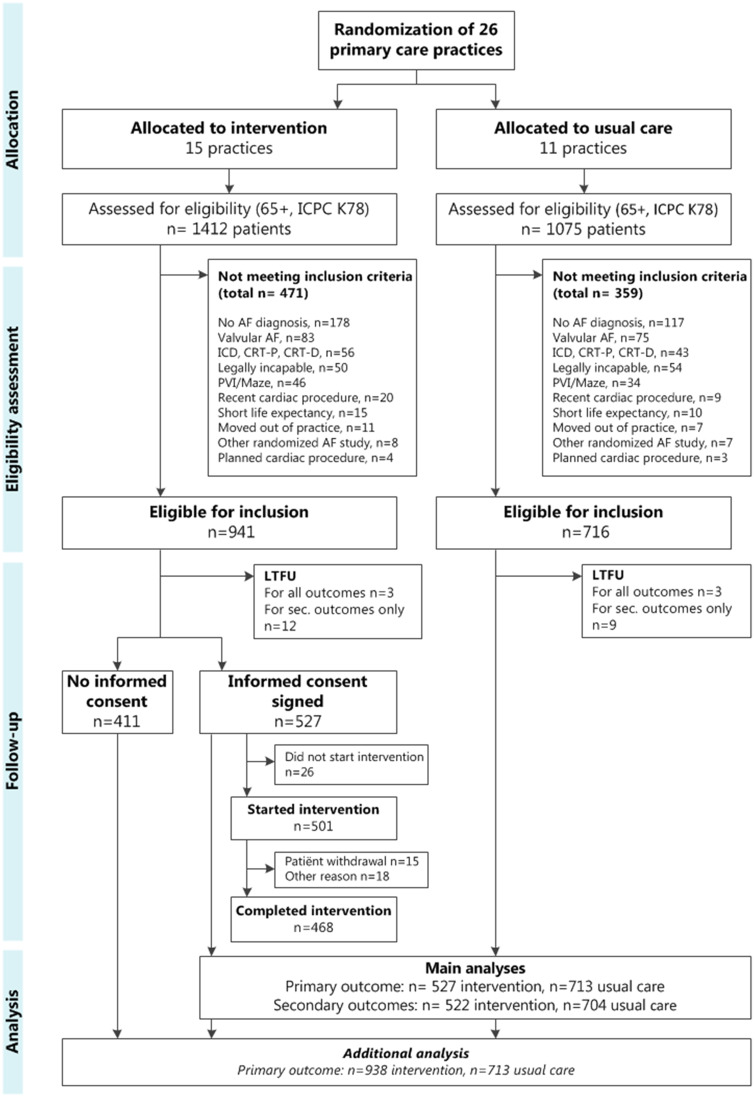
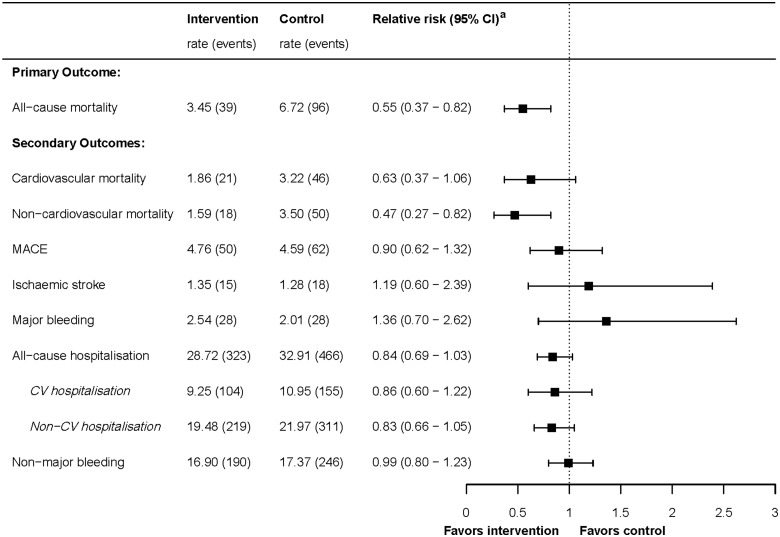
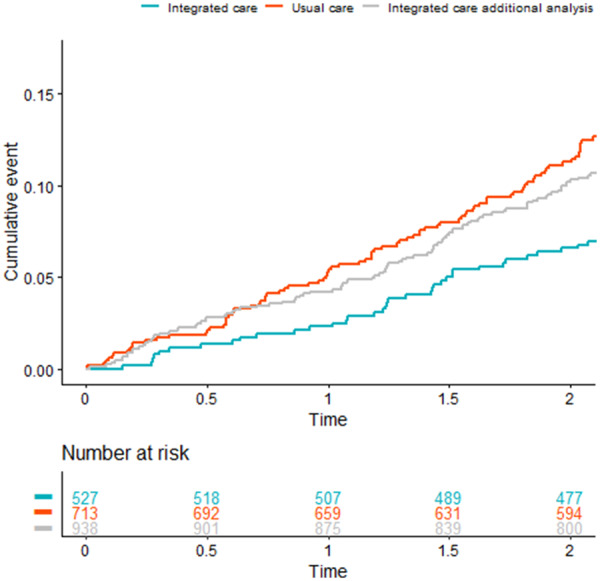
The ALL-IN trial was a cluster randomized, open-label, pragmatic non-inferiority trial performed in primary care practices in the Netherlands. We randomized 26 practices: 15 to the integrated care intervention and 11 to usual care. The integrated care intervention consisted of (i) quarterly AF check-ups by trained nurses in primary care, also focusing on possibly interfering comorbidities, (ii) monitoring of anticoagulation therapy in primary care, and finally (iii) easy-access availability of consultations from cardiologists and anticoagulation clinics. The primary endpoint was all-cause mortality during 2 years of follow-up. In the intervention arm, 527 out of 941 eligible AF patients aged ≥65 years provided informed consent to undergo the intervention. These 527 patients were compared with 713 AF patients in the control arm receiving usual care. Median age was 77 (interquartile range 72-83) years. The all-cause mortality rate was 3.5 per 100 patient-years in the intervention arm vs. 6.7 per 100 patient-years in the control arm [adjusted hazard ratio (HR) 0.55; 95% confidence interval (CI) 0.37-0.82]. For non-cardiovascular mortality, the adjusted HR was 0.47 (95% CI 0.27-0.82). For other adverse events, no statistically significant differences were observed.
In this cluster randomized trial, integrated care for elderly AF patients in primary care showed a 45% reduction in all-cause mortality when compared with usual care.
评估在初级保健中是否能够安全地协调房颤(AF)的综合护理。
ALL-IN试验是一项在荷兰初级保健机构中进行的整群随机、开放标签、实用性非劣效性试验。我们将26个机构随机分组:15个接受综合护理干预,11个接受常规护理。综合护理干预包括:(i)由初级保健中经过培训的护士每季度进行一次房颤检查,同时关注可能产生干扰的合并症;(ii)在初级保健中监测抗凝治疗;最后,(iii)方便患者获得心脏病专家和抗凝门诊的会诊。主要终点是随访2年期间的全因死亡率。在干预组中,941例年龄≥65岁的符合条件的房颤患者中有527例提供了知情同意以接受干预。将这527例患者与接受常规护理的对照组中的713例房颤患者进行比较。中位年龄为77岁(四分位间距72 - 83岁)。干预组的全因死亡率为每100患者年3.5例,而对照组为每100患者年6.7例[调整后风险比(HR)0.55;95%置信区间(CI)0.37 - 0.82]。对于非心血管死亡率,调整后的HR为0.47(95% CI 0.27 - 0.82)。对于其他不良事件,未观察到统计学上的显著差异。
在这项整群随机试验中,与常规护理相比,初级保健中针对老年房颤患者的综合护理使全因死亡率降低了45%。