School of Public Health, University College Cork, Cork, Ireland; Irish Centre for Maternal and Child Health Research (INFANT), Cork University Maternity Hospital, University College Cork, Cork, Ireland.
Irish Centre for Maternal and Child Health Research (INFANT), Cork University Maternity Hospital, University College Cork, Cork, Ireland; Department of Obstetrics & Gynaecology, Cork University Maternity Hospital, University College Cork, Cork, Ireland.
Am J Obstet Gynecol. 2020 Sep;223(3):427.e1-427.e14. doi: 10.1016/j.ajog.2020.02.031. Epub 2020 Feb 26.
Stillbirth is a devastating adverse pregnancy outcome that may occur without any obvious reason or may occur in the context of fetal growth restriction, preeclampsia, or other obstetric complications. There is increasing evidence that women who experience stillbirths are at greater risk of long-term cardiovascular disease, but little is known about their risk of chronic kidney disease and end-stage renal disease. We conducted the largest study to date to investigate the subsequent risk of maternal chronic kidney disease and end-stage renal disease following stillbirth.
To identify whether pregnancy complicated by stillbirth is associated with subsequent risk of maternal chronic kidney disease and end-stage renal disease, independent of underlying medical or obstetric comorbidities.
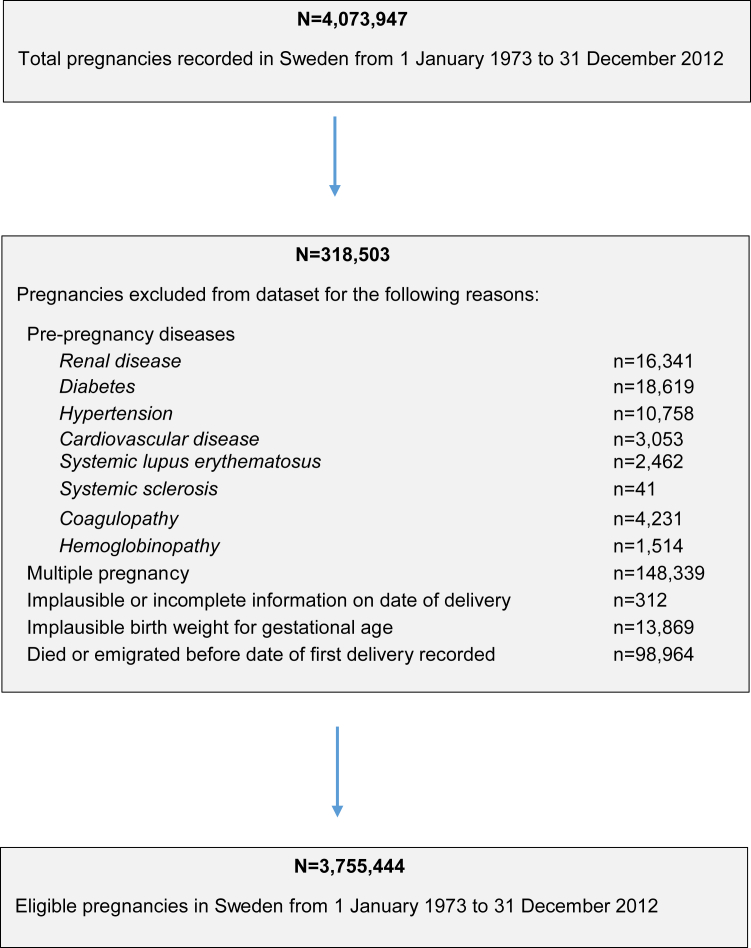
STUDY DESIGN/METHODS: We conducted a population-based cohort study using nationwide data from the Swedish Medical Birth Register, National Patient Register, and Swedish Renal Register. We included all women who had live births and stillbirths from 1973 to 2012, with follow-up to 2013. Women with preexisting renal disease were excluded. Cox proportional hazard regression models were used to estimate adjusted hazard ratios and 95% confidence intervals for associations between stillbirth and maternal chronic kidney disease and end-stage renal disease respectively. We controlled for maternal age, year of delivery, country of origin, parity, body mass index, smoking, gestational diabetes, preeclampsia, and small for gestational age deliveries. Women who had a history of medical comorbidities, which may predispose to renal disease (prepregnancy cardiovascular disease, hypertension, diabetes, lupus, systemic sclerosis, hemoglobinopathy, or coagulopathy), were excluded from the main analysis and examined separately.
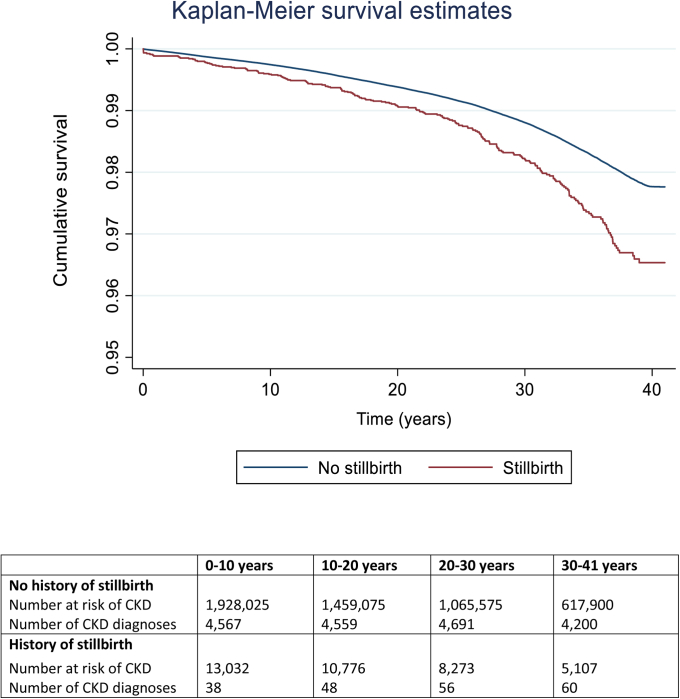
There were 1,941,057 unique women who had 3,755,444 singleton pregnancies, followed up over 42,313,758 person-years. The median follow-up time was 20.7 years (interquartile range, 9.9-30.0 years). 13,032 women (0.7%) had at least 1 stillbirth. Women who had experienced at least 1 stillbirth had a greater risk of developing chronic kidney disease (adjusted hazard ratio, 1.26; 95% confidence interval, 1.09-1.45) and end-stage renal disease (adjusted hazard ratio, 2.25; 95% confidence interval, 1.55-3.25) compared with women who only had live births. These associations persisted after removing all stillbirths that occurred in the context of preeclampsia, and small for gestational age or congenital malformations (for chronic kidney disease, adjusted hazard ratio, 1.33; 95% confidence interval, 1.13-1.57; for end-stage renal disease, adjusted hazard ratio, 2.95; 95% confidence interval, CI 1.86-4.68). There was no significant association observed between stillbirth and either chronic kidney disease or end-stage renal disease in women who had preexisting medical comorbidities (chronic kidney disease, adjusted hazard ratio, 1.13; 95% confidence interval, 0.73-1.75 or end-stage renal disease, adjusted hazard ratio, 1.49; 95% confidence interval, 0.78-2.85).
Women who have a history of stillbirth may be at increased risk of chronic kidney disease and end-stage renal disease compared with women who have only had live births. This association persists independently of preeclampsia, and small for gestational age, maternal smoking, obesity, and medical comorbidities. Further research is required to determine whether affected women would benefit from closer surveillance and follow-up for future renal disease.
死胎是一种严重的不良妊娠结局,可能没有任何明显原因发生,也可能发生在胎儿生长受限、子痫前期或其他产科并发症的情况下。越来越多的证据表明,经历过死胎的女性患长期心血管疾病的风险更高,但对于她们患慢性肾脏病和终末期肾病的风险知之甚少。我们进行了迄今为止最大的研究,以调查死胎后女性患慢性肾脏病和终末期肾病的后续风险。
确定妊娠合并死胎是否与随后发生慢性肾脏病和终末期肾病的风险相关,而不考虑潜在的医学或产科合并症。
研究设计/方法:我们使用瑞典全国性数据,包括来自瑞典医学出生登记处、国家患者登记处和瑞典肾脏登记处的数据,进行了一项基于人群的队列研究。我们纳入了 1973 年至 2012 年期间活产和死产的所有女性,随访至 2013 年。排除了有预先存在的肾脏疾病的女性。使用 Cox 比例风险回归模型估计了死胎与慢性肾脏病和终末期肾病的关联的调整后的危险比和 95%置信区间。我们控制了母亲的年龄、分娩年份、原籍国、产次、体重指数、吸烟、妊娠期糖尿病、子痫前期和小于胎龄儿分娩。有预先存在的医疗合并症(可能导致肾脏疾病的妊娠前心血管疾病、高血压、糖尿病、狼疮、系统性硬化症、血红蛋白病或凝血障碍)病史的女性被排除在主要分析之外,并分别进行了检查。
共有 1941057 名女性有 3755444 次单胎妊娠,随访时间超过 42313788 人年。中位随访时间为 20.7 年(四分位距,9.9-30.0 年)。13032 名女性(0.7%)至少有一次死胎。与只有活产的女性相比,经历过至少一次死胎的女性发生慢性肾脏病(调整后的危险比,1.26;95%置信区间,1.09-1.45)和终末期肾病(调整后的危险比,2.25;95%置信区间,1.55-3.25)的风险更高。在去除子痫前期、小于胎龄儿或先天性畸形相关的所有死胎后,这些关联仍然存在(对于慢性肾脏病,调整后的危险比,1.33;95%置信区间,1.13-1.57;对于终末期肾病,调整后的危险比,2.95;95%置信区间,1.86-4.68)。在有预先存在的医疗合并症的女性中,死胎与慢性肾脏病或终末期肾病之间没有显著关联(慢性肾脏病,调整后的危险比,1.13;95%置信区间,0.73-1.75;或终末期肾病,调整后的危险比,1.49;95%置信区间,0.78-2.85)。
与只有活产的女性相比,有死胎史的女性可能患有慢性肾脏病和终末期肾病的风险增加。这种关联独立于子痫前期、小于胎龄儿、母亲吸烟、肥胖和医疗合并症而存在。需要进一步研究以确定受影响的女性是否会受益于更密切的监测和随访以预防未来的肾脏疾病。