Department of Surgery, Penn State Hershey College of Medicine and Milton S. Hershey Medical Center, Hershey, Pennsylvania, USA.
Department of Surgery, Eastern Regional Hospital, Koforidua, Ghana.
BMJ Open Gastroenterol. 2020 Feb 17;7(1):e000350. doi: 10.1136/bmjgast-2019-000350. eCollection 2020.
In 2013, peptic ulcer disease (PUD) caused over 300 000 deaths globally. Low-income and middle-income countries are disproportionately affected. However, there is limited information regarding risk factors of perioperative mortality rates in these countries.
To assess perioperative mortality rates from complicated PUD in Africa and associated risk factors.
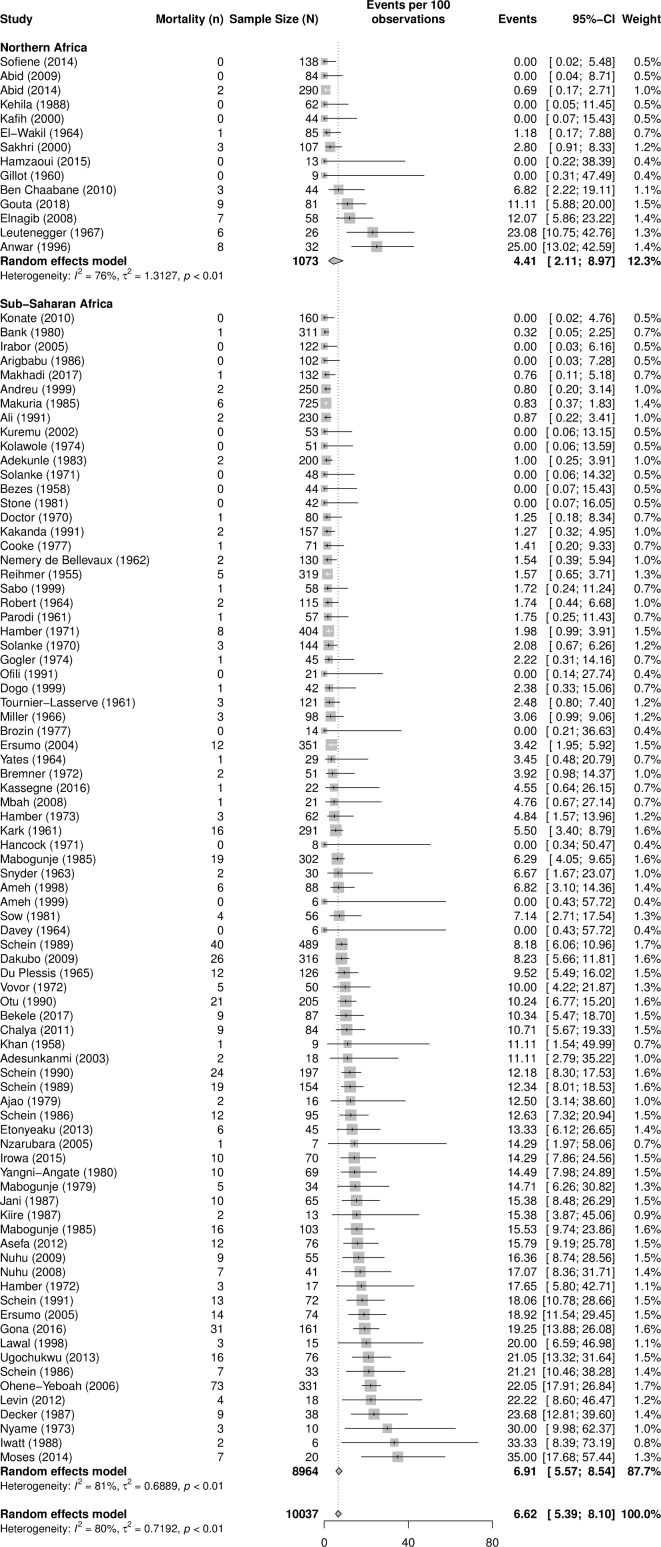
We performed a systematic review and a random-effect meta-analysis of literature describing surgical management of complicated PUD in Africa. We used subgroup analysis and meta-regression analyses to investigate sources of variations in the mortality rates and to assess the risk factors contributing to mortality.
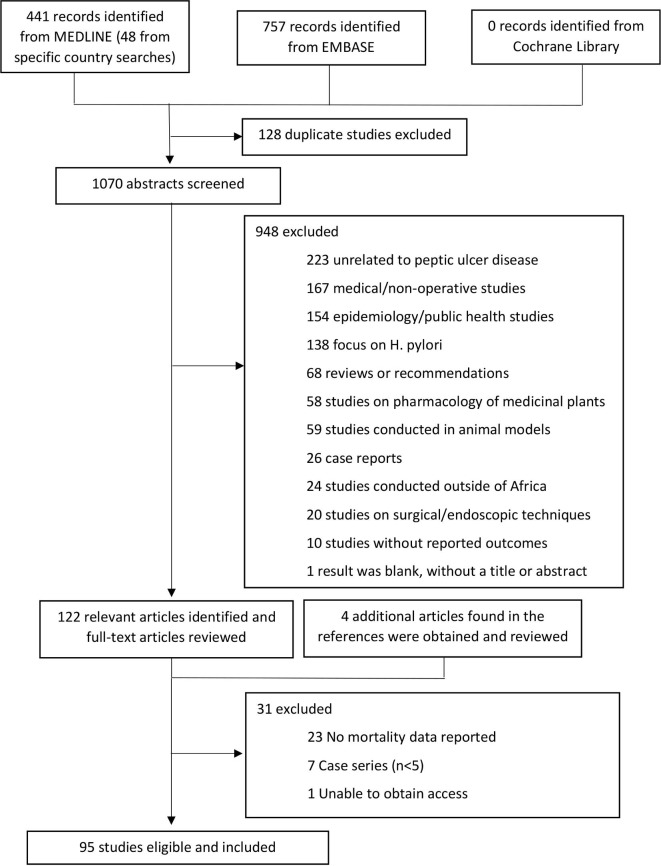
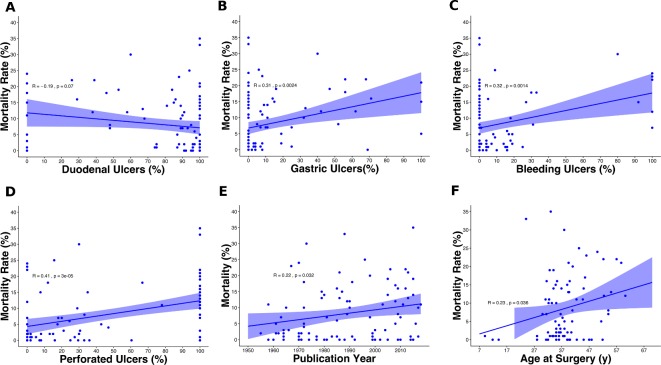
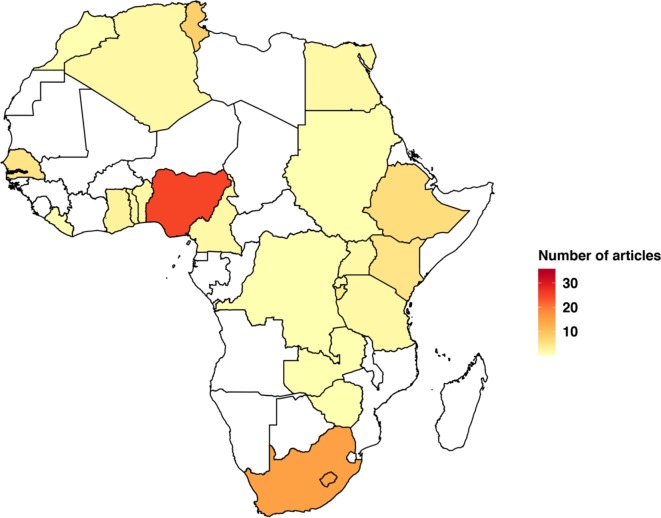
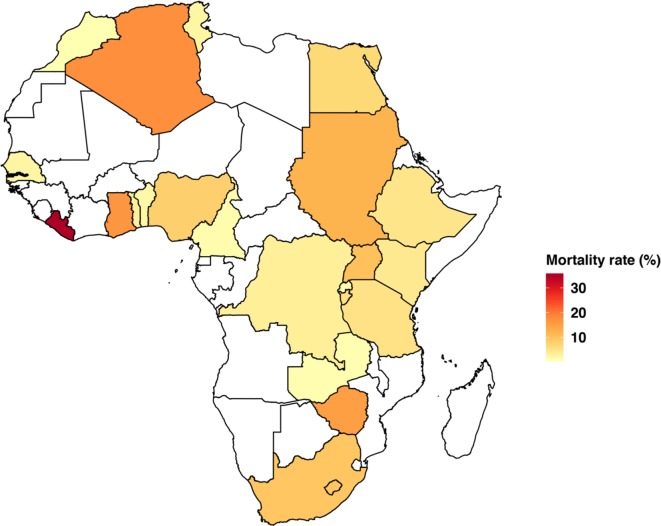
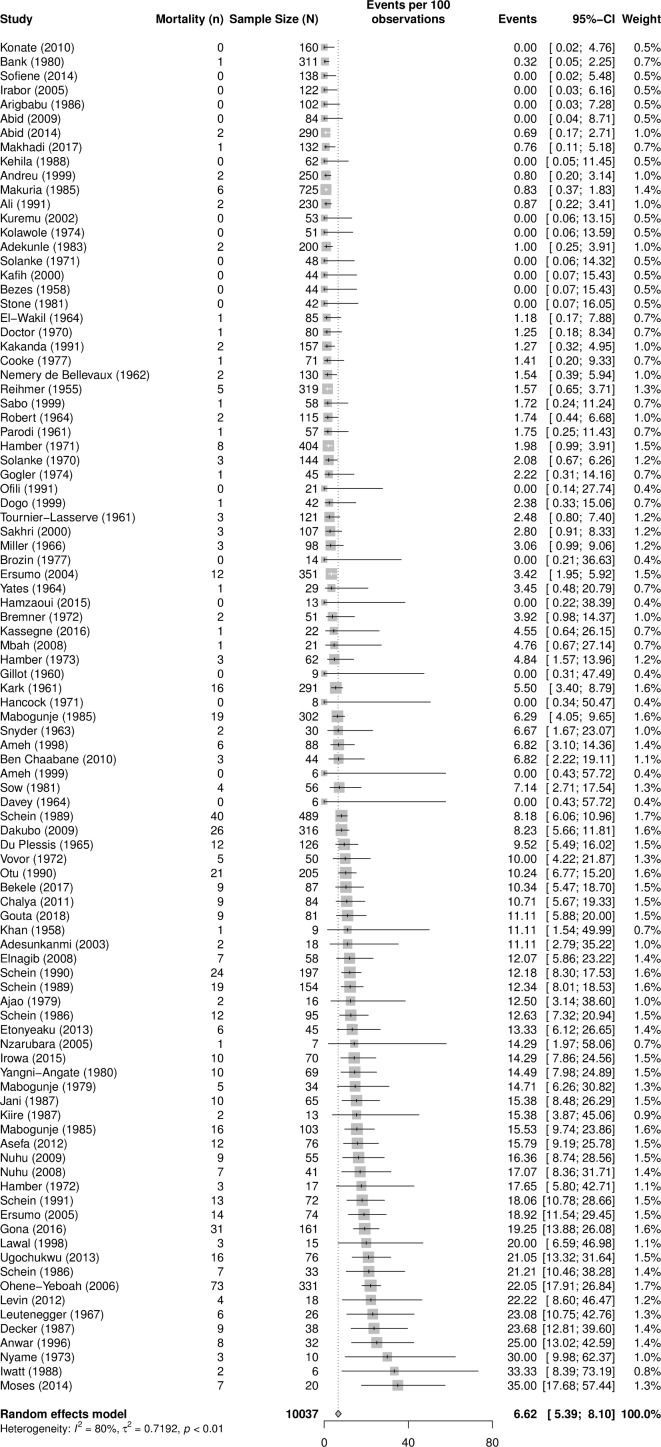
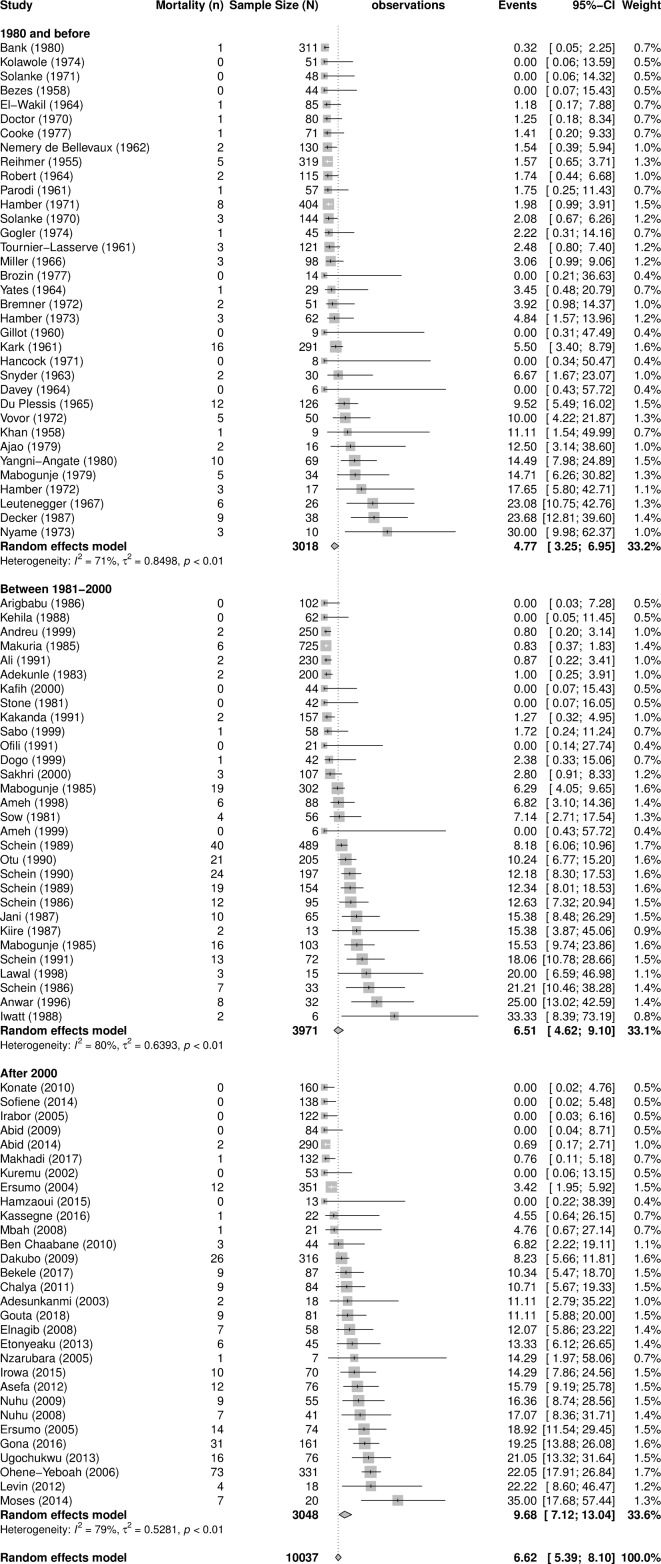
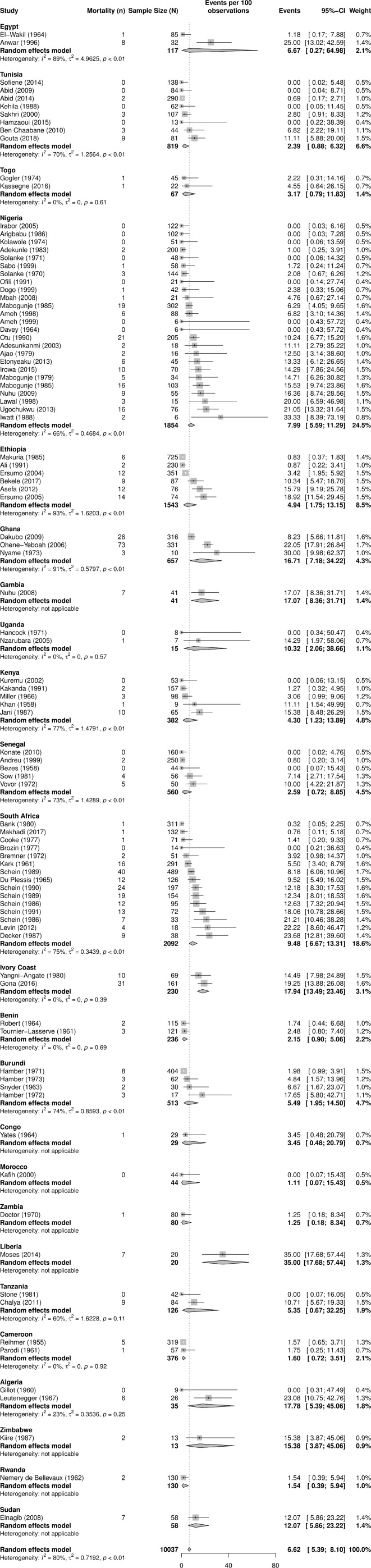
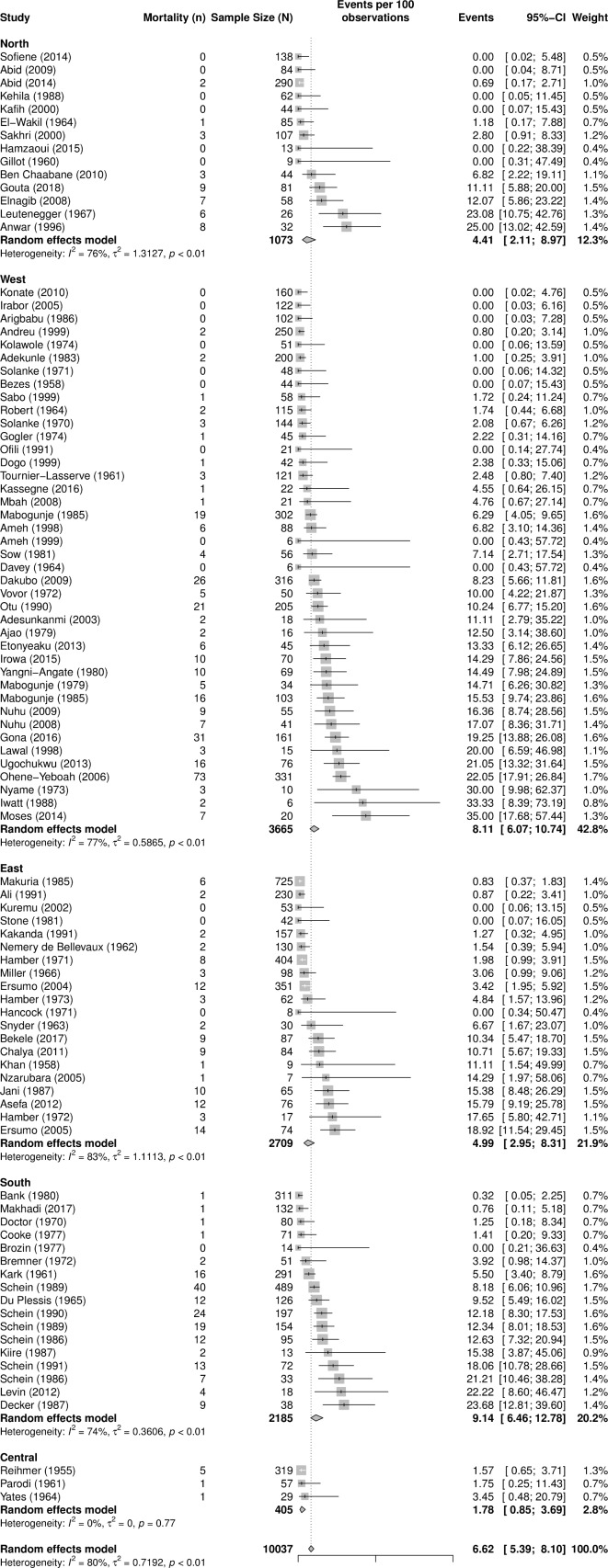
From 95 published reports, 10 037 patients underwent surgery for complicated PUD. The majority of the ulcers (78%) were duodenal, followed by gastric (14%). Forty-one per cent of operations were for perforation, 22% for obstruction and 9% for bleeding. The operations consisted of vagotomy (38%), primary repair (34%), resection and reconstruction (12%), and drainage procedures (6%). The overall PUD mortality rate was 6.6% (95% CI 5.4% to 8.1%). It increased to 9.7% (95% CI 7.1 to 13.0) when we limited the analysis to studies published after the year 2000. The correlation was higher between perforated PUD and mortality rates (r=0.41, p<0.0001) than for bleeding PUD and mortality rates (r=0.32, p=0.001). Non-significant differences in mortality rates existed between sub-Saharan Africa (SSA) and North Africa and within SSA.
Perioperative mortality rates from complicated PUD in Africa are substantially high and could be increasing over time, and there are possible regional differences.
2013 年,全球有超过 30 万人死于消化性溃疡病(PUD)。低收入和中等收入国家的受影响程度不成比例。然而,关于这些国家围手术期死亡率的风险因素的信息有限。
评估非洲并发 PUD 的围手术期死亡率及其相关风险因素。
我们对描述非洲并发 PUD 手术治疗的文献进行了系统评价和随机效应荟萃分析。我们使用亚组分析和荟萃回归分析来调查死亡率变化的来源,并评估导致死亡率的风险因素。
从 95 篇已发表的报告中,有 10037 名患者因并发 PUD 接受了手术。大多数溃疡(78%)是十二指肠溃疡,其次是胃溃疡(14%)。41%的手术是为了穿孔,22%是为了梗阻,9%是为了出血。手术包括迷走神经切断术(38%)、一期修复术(34%)、切除术和重建术(12%)以及引流术(6%)。总体 PUD 死亡率为 6.6%(95%CI 5.4%至 8.1%)。当我们将分析仅限于 2000 年后发表的研究时,死亡率增加到 9.7%(95%CI 7.1%至 13.0%)。穿孔性 PUD 与死亡率的相关性高于出血性 PUD 与死亡率的相关性(r=0.41,p<0.0001)。撒哈拉以南非洲(SSA)与北非以及 SSA 内部的死亡率之间没有显著差异。
非洲并发 PUD 的围手术期死亡率相当高,并且可能随着时间的推移而增加,而且可能存在地区差异。