Kim Do Yeon, Kwon Hee, Nam Ki-Woong, Lee Yongseok, Kwon Hyung-Min, Chung Young Seob
Department of Neurology, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Republic of Korea.
Medical Corps, Republic of Korea Navy, Jeju Island, Republic of Korea.
J Med Internet Res. 2020 Feb 27;22(2):e15377. doi: 10.2196/15377.
Advances in mobile health (mHealth) have enabled systematic and continuous management of patients with chronic diseases.
We developed a smartphone-based mHealth system and aimed to evaluate its effects on health behavior management and risk factor control in stroke patients.
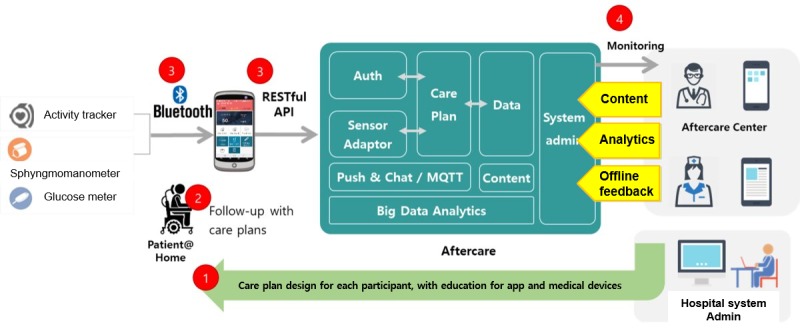
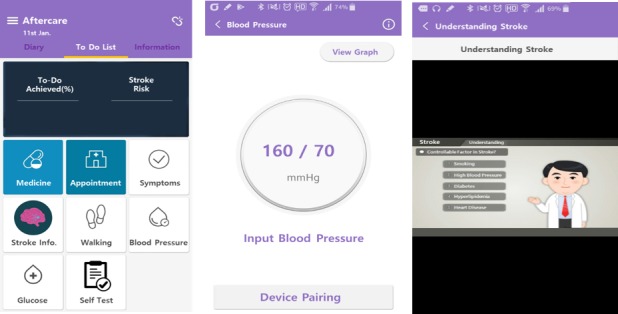
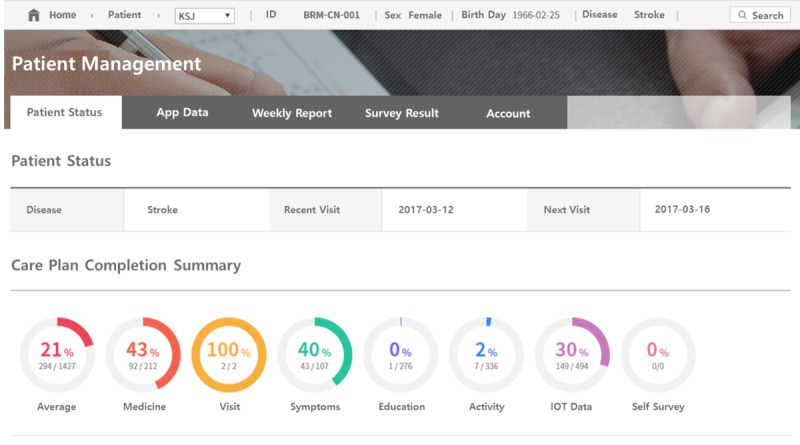
With a multifaceted stroke aftercare management system that included exercise, medication, and educational materials, we performed a 12-week single-arm intervention among eligible poststroke patients in the stroke clinic from September to December 2016. The intervention consisted of (1) regular blood pressure (BP), blood glucose, and physical activity measurements; (2) stroke education; (3) an exercise program; (4) a medication program; and (5) feedback on reviewing of records by clinicians. Clinical assessments consisted of the stroke awareness score, Beck Depression Inventory-II (BDI), EuroQol-5 Dimensions (EQ-5D), and BP at visit 1 (baseline), visit 2 (4 weeks), and visit 3 (12 weeks). Temporal differences in the parameters over 12 weeks were investigated with repeated-measures analysis of variance. Changes in medication adherence at visit 1-2 (from visit 1 to visit 2) and visit 2-3 (from visit 2 to visit 3) were compared. System satisfaction was evaluated with a self-questionnaire using a 5-point Likert scale at visit 3.
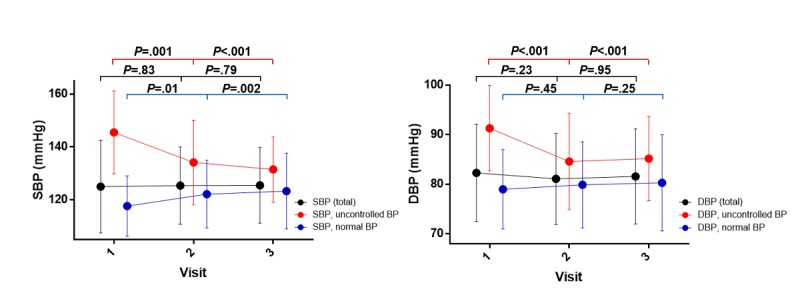
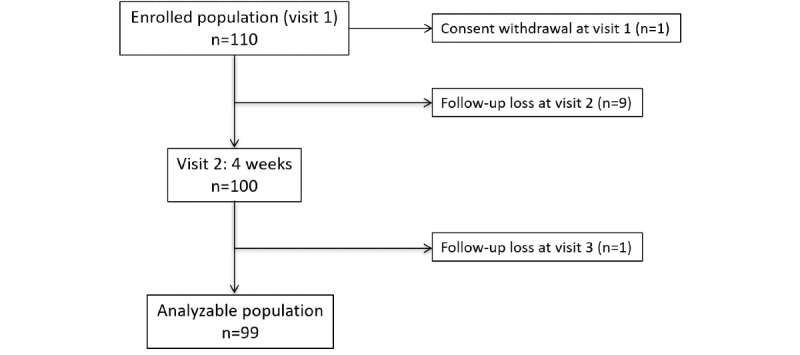
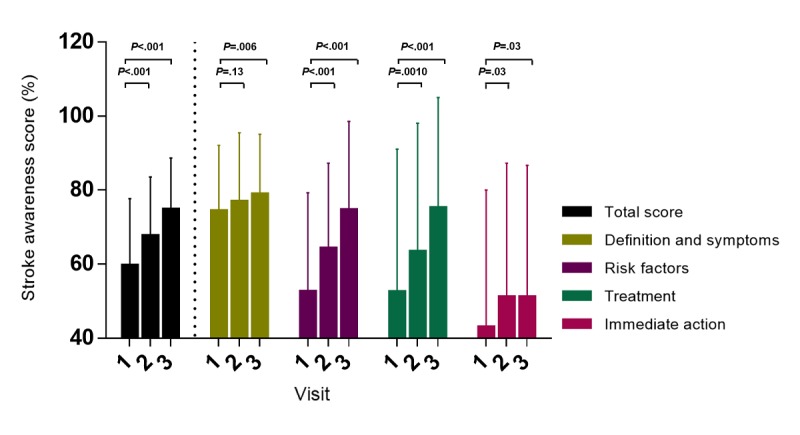
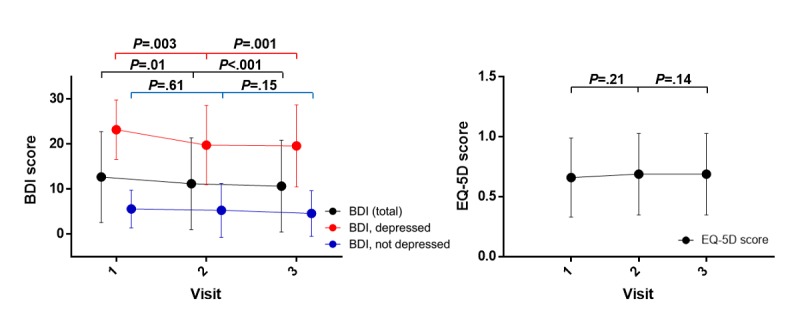
The study was approved by the Institutional Review Board in September 2016, and participants were enrolled from September to December 2016. Among the 110 patients enrolled for the study, 99 were included in our analyses. The mean stroke awareness score (baseline: 59.6 [SD 18.1]; 4 weeks: 67.6 [SD 16.0], P<.001; 12 weeks: 74.7 [SD 14.0], P<.001) and BDI score (baseline: 12.7 [SD 10.1]; 4 weeks: 11.2 [SD 10.2], P=.01; 12 weeks: 10.7 [SD 10.2], P<.001) showed gradual improvement; however, no significant differences were found in the mean EQ-5D score (baseline: 0.66 [SD 0.33]; 4 weeks: 0.69 [SD 0.34], P=.01; 12 weeks: 0.69 [SD 0.34], P<.001). Twenty-six patients who had uncontrolled BP at baseline had -13.92 mmHg (P=.001) and -6.19 mmHg (P<.001) reductions on average in systolic and diastolic BP, respectively, without any antihypertensive medication change. Medication compliance was better at visit 2-3 (60.9% [SD 37.2%]) than at visit 1-2 (47.8% [SD 38.7%], P<.001).
Awareness of stroke, depression, and BP was enhanced when using the smartphone-based mHealth system. Emerging mHealth techniques have potential as new nonpharmacological secondary prevention methods because of their ubiquitous access, near real-time responsiveness, and comparatively lower cost.
移动健康(mHealth)的进步使得对慢性病患者进行系统且持续的管理成为可能。
我们开发了一种基于智能手机的移动健康系统,旨在评估其对中风患者健康行为管理和危险因素控制的影响。
借助一个包含运动、药物治疗和教育材料的多方面中风康复后管理系统,我们于2016年9月至12月在中风诊所对符合条件的中风后患者进行了为期12周的单臂干预。干预措施包括:(1)定期测量血压(BP)、血糖和身体活动情况;(2)中风教育;(3)一个运动计划;(4)一个药物治疗计划;以及(5)临床医生对记录复查的反馈。临床评估包括中风知晓评分、贝克抑郁量表第二版(BDI)、欧洲五维健康量表(EQ - 5D),以及在第1次就诊(基线)、第2次就诊(4周)和第3次就诊(12周)时测量的血压。通过重复测量方差分析研究12周内这些参数的时间差异。比较第1 - 2次就诊(从第1次就诊到第2次就诊)和第2 - 3次就诊(从第2次就诊到第3次就诊)期间药物依从性的变化。在第3次就诊时使用5点李克特量表通过自填问卷评估系统满意度。
该研究于2016年9月获得机构审查委员会批准,参与者于2016年9月至12月招募。在纳入研究的110例患者中,99例纳入我们的分析。平均中风知晓评分(基线:59.6 [标准差18.1];4周:67.6 [标准差16.0],P <.001;12周:74.7 [标准差14.0],P <.001)和BDI评分(基线:12.7 [标准差10.1];4周:11.2 [标准差10.2],P =.01;12周:10.7 [标准差10.2],P <.001)显示出逐渐改善;然而,平均EQ - 5D评分无显著差异(基线:0.66 [标准差0.33];4周:0.69 [标准差0.34],P =.01;12周:0.69 [标准差0.34],P <.001)。26例基线时血压未得到控制的患者,在未改变任何抗高血压药物的情况下,收缩压平均降低了 - 13.92 mmHg(P =.001),舒张压平均降低了 - 6.19 mmHg(P <.001)。第2 - 3次就诊时的药物依从性(60.9% [标准差37.2%])优于第1 - 2次就诊时(47.8% [标准差38.7%],P <.001)。
使用基于智能手机的移动健康系统可提高对中风、抑郁和血压的认知。新兴的移动健康技术因其无处不在的接入性、近乎实时的响应性和相对较低的成本,有望成为新的非药物二级预防方法。