Kim Dohyung, Jo Hyunmin, Lee Younsuk, Kim Kyoung Ok
Department of Anesthesiology and Pain Medicine, Dongguk University Ilsan Hospital, Goyang, Korea.
Acute Crit Care. 2020 Feb;35(1):10-15. doi: 10.4266/acc.2019.00745. Epub 2020 Feb 29.
As the average life expectancy increases, anesthesiologists confront unique challenges in the perioperative care of elderly patients who have significant comorbidities. In this study, we evaluated Elixhauser comorbidity measures-based risk factors associated with 30day mortality in patients aged 66 years and older who underwent femur fracture surgery.
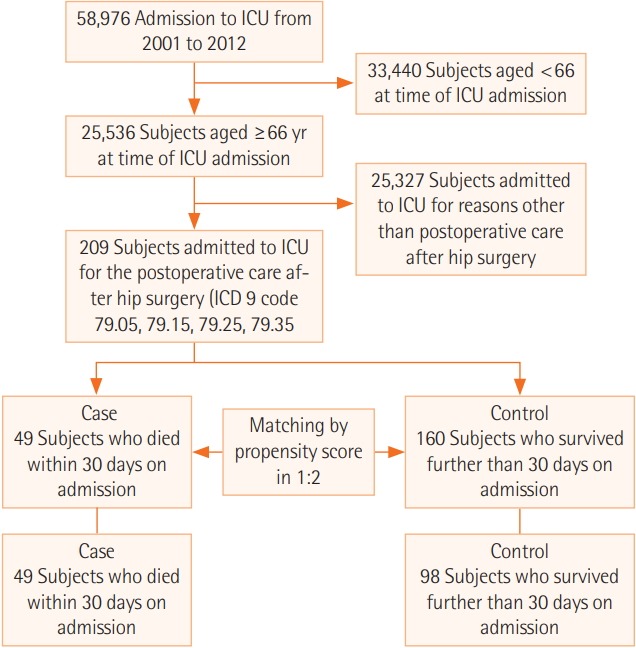
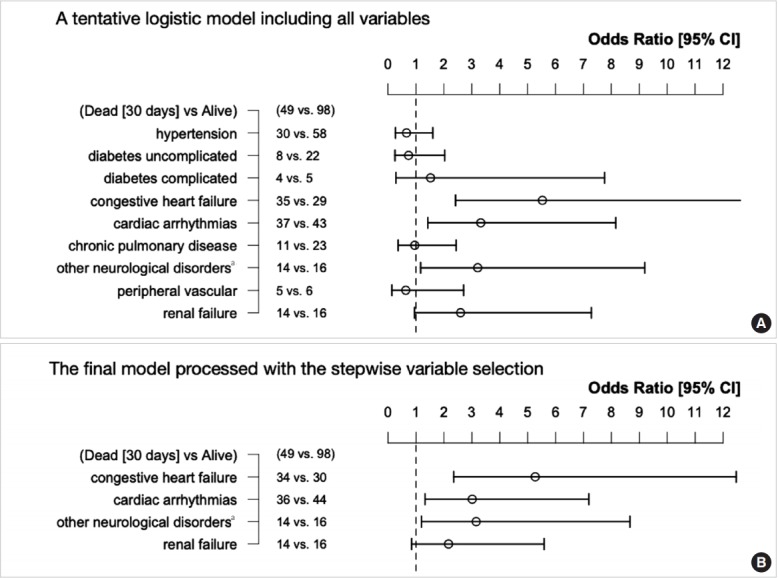
We used the Medical Information Mart for Intensive Care III which contains the medical records of patients admitted to the intensive care unit (ICU) at Beth Israel Deaconess Medical Center in the United States between 2001 and 2012 to identify patients admitted to the ICU after femur fracture surgery (n=209). Patients who died within 30 days of admission (case group, n=49) were propensity score-matched to patients who did not (control group, n=98). The variables for matching were age, sex, race, anemia (hemoglobin ≤10 g/dl), and malignancy. We attempted to explain mortality via nine independent factors: hypertension, uncomplicated diabetes, complicated diabetes, congestive heart failure (CHF), cardiac arrhythmias, chronic pulmonary disease, renal failure, neurological disorders other than paralysis, and peripheral vascular disease.
Logistic regression identified three significant risk factors: CHF, arrhythmias, and neurological disorders other than paralysis. The odds ratio (OR) for the 30-day mortality of CHF was 4.99 (95% confidence interval [CI], 2.18 to 12.06). The equivalent ORs for cardiac arrhythmias and neurological disorders other than paralysis were 2.61 (95% CI, 1.14 to 6.21) and 2.40 (95% CI, 0.95 to 6.48), respectively.
Identifying patients with these risk factors (CHF, arrhythmias, and neurological disorders other than paralysis) will assist clinicians with perioperative planning and provide caregivers with valuable information for decision-making.
随着平均预期寿命的增加,麻醉医生在患有严重合并症的老年患者围手术期护理中面临着独特的挑战。在本研究中,我们评估了基于埃利克斯豪泽合并症测量法的、与66岁及以上接受股骨骨折手术患者30天死亡率相关的风险因素。
我们使用重症监护医疗信息集市III,其包含2001年至2012年期间在美国贝斯以色列女执事医疗中心重症监护病房(ICU)住院患者的医疗记录,以识别股骨骨折手术后入住ICU的患者(n = 209)。在入院30天内死亡的患者(病例组,n = 49)与未死亡的患者(对照组,n = 98)进行倾向评分匹配。匹配变量为年龄、性别、种族、贫血(血红蛋白≤10 g/dl)和恶性肿瘤。我们试图通过九个独立因素解释死亡率:高血压、非复杂性糖尿病、复杂性糖尿病、充血性心力衰竭(CHF)、心律失常、慢性肺病、肾衰竭、除瘫痪外的神经疾病和外周血管疾病。
逻辑回归确定了三个显著风险因素:CHF、心律失常和除瘫痪外的神经疾病。CHF 30天死亡率的比值比(OR)为4.99(95%置信区间[CI],2.18至12.06)。心律失常和除瘫痪外的神经疾病的等效OR分别为2.61(95%CI,1.14至6.21)和2.40(95%CI,0.95至6.48)。
识别具有这些风险因素(CHF、心律失常和除瘫痪外的神经疾病)的患者将有助于临床医生进行围手术期规划,并为护理人员提供有价值的决策信息。