Kim Si Youn, Choi Munseok, Hwang Ho Kyoung, Rho Seoung Yoon, Lee Woo Jung, Kang Chang Moo
Yonsei University College of Medicine, Seoul 03722, Korea.
Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Yonsei University College of Medicine, Seoul 03722, Korea.
J Clin Med. 2020 Mar 4;9(3):689. doi: 10.3390/jcm9030689.
Investigate whether intraoperative transfusion is a negative prognostic factor for oncologic outcomes of resected pancreatic cancer.
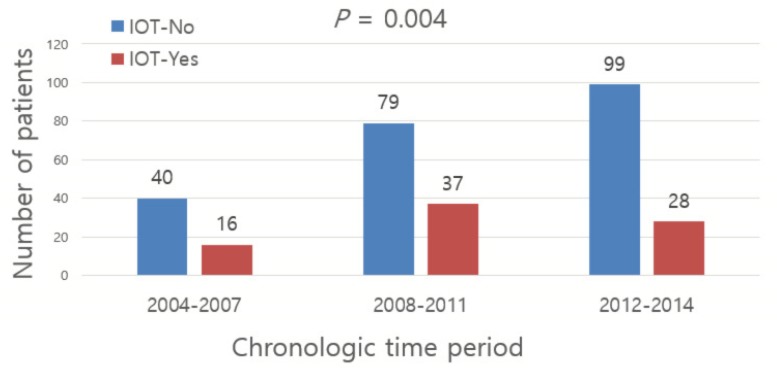
From June 2004 to January 2014, the medical records of 305 patients were retrospectively reviewed, who underwent pancreatoduodenectomy, pylorus preserving pancreatoduodenectomy, total pancreatectomy, distal pancreatectomy for pancreatic cancer. Patients diagnosed with metastatic disease (n = 3) and locally advanced diseases (n = 15) were excluded during the analysis, and total of 287 patients were analyzed.
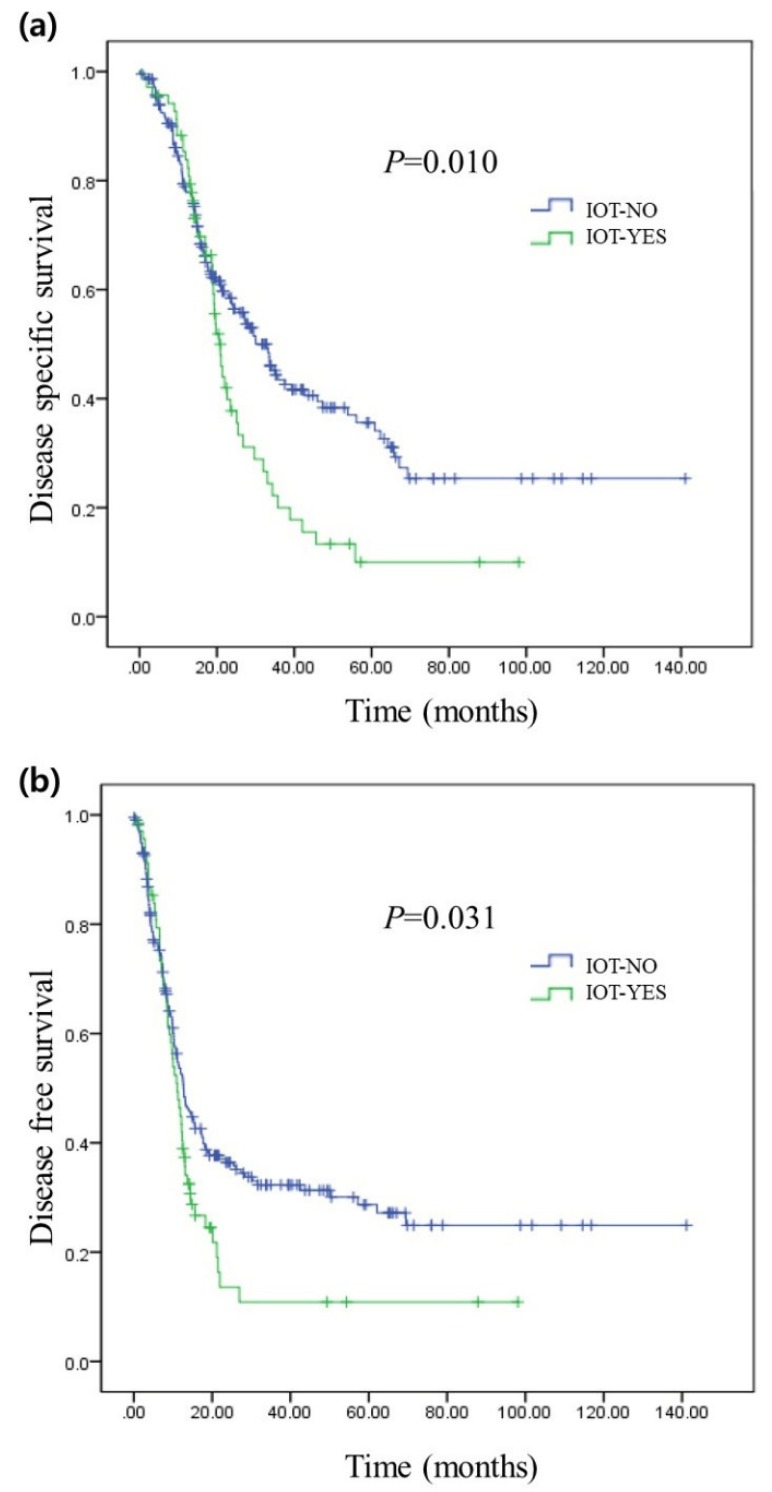
The recurrence and disease-specific survival rates of the patients who received intraoperative transfusion showed poorer survival outcomes compared to those who did not ( = 0.031, = 0.010). Through multivariate analysis, T status (HR (hazard ratio) = 2.04, [95% CI (confidence interval): 1.13-3.68], = 0.018), N status (HR = 1.46 [95% CI: 1.00-2.12], = 0.045), adjuvant chemotherapy (HR = 0.51, [95% CI: 0.35-0.75], = 0.001), intraoperative transfusion (HR = 1.94 [95% CI: 1.23-3.07], = 0.004) were independent prognostic factors of disease-specific survival after surgery. As well, adjuvant chemotherapy (HR = 0.67, [95% CI: 0.46-0.97], = 0.035) was independently associated with tumor recurrence. Estimated blood loss was one of the most powerful factors associated with intraoperative transfusion ( < 0.001).
Intraoperative transfusion can be considered as an independent prognostic factor of resected pancreatic cancer. As well, it can be avoided by following strict transfusion policy and using advanced surgical techniques to minimize bleeding during surgery.
研究术中输血是否是切除的胰腺癌肿瘤学预后的负面预测因素。
回顾性分析2004年6月至2014年1月期间305例行胰十二指肠切除术、保留幽门的胰十二指肠切除术、全胰切除术、胰腺癌远端胰腺切除术患者的病历。分析时排除诊断为转移性疾病(n = 3)和局部晚期疾病(n = 15)的患者,共分析287例患者。
与未接受术中输血的患者相比,接受术中输血的患者的复发率和疾病特异性生存率显示出较差的生存结果(P = 0.031,P = 0.010)。通过多因素分析,T分期(风险比(HR)= 2.04,[95%置信区间(CI):1.13 - 3.68],P = 0.018)、N分期(HR = 1.46 [95% CI:1.00 - 2.12],P = 0.045)、辅助化疗(HR = 0.51,[95% CI:0.35 - 0.75],P = 0.001)、术中输血(HR = 1.94 [95% CI:1.23 - 3.07],P = 0.004)是术后疾病特异性生存的独立预后因素。同样,辅助化疗(HR = 0.67,[95% CI:0.46 - 0.97],P = 0.035)与肿瘤复发独立相关。估计失血量是与术中输血相关的最有力因素之一(P < 0.001)。
术中输血可被视为切除的胰腺癌的独立预后因素。此外,遵循严格的输血政策并使用先进的手术技术以尽量减少手术中的出血可避免术中输血。