Awotoye Josephine, Fashanu Oluwaseun E, Lutsey Pamela L, Zhao Di, O'Neal Wesley T, Michos Erin D
Department of Biology, University of Minnesota, Minneapolis, Minnesota, USA.
Department of Medicine, Saint Agnes Hospital, Baltimore, Maryland, USA.
Open Heart. 2020 Feb 20;7(1):e001080. doi: 10.1136/openhrt-2019-001080. eCollection 2020.
Venous thromboembolism (VTE) is associated with significant morbidity and mortality. Resting heart rate (RHR), which may be modifiable through lifestyle changes, has been shown to be associated with cardiovascular disease risk and with inflammatory markers that have been predictive of VTE incidence.
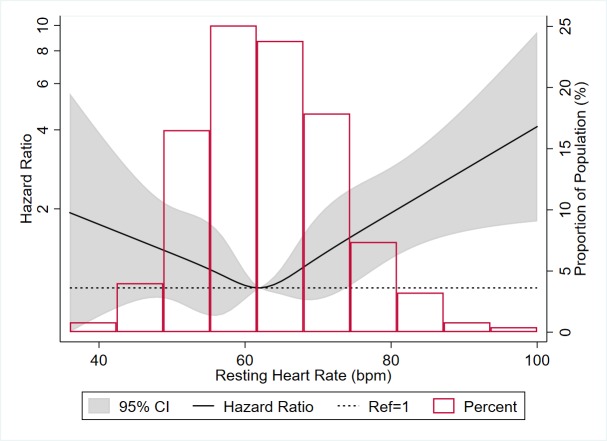
We examined whether RHR is also associated with VTE incidence independent of these risk factors. We studied 6479 Multi-Ethnic Study of Atherosclerosis participants free from clinical VTE at baseline who had baseline RHR ascertained by 12-lead ECG. VTE events were recorded from hospital records and death certificates using International Classification of Diseases (ICD)-9 and ICD-10 codes. We categorised RHR as <60, 60-69, 70-79 and ≥80 bpm. We used Cox hazard models to determine the association of incident VTE by RHR.
Participants had mean (SD) age of 62 (10) years and RHR of 63 (10) bpm. RHR was cross-sectionally correlated with multiple inflammatory and coagulation factors. There were 236 VTE cases after a median follow-up of 14 years. Compared with those with RHR<60 bpm, the HR (95% CI) for incident VTE for RHR≥80 bpm was 2.08 (1.31 to 3.30), after adjusting for demographics, physical activity, smoking, diabetes and use of atrioventricular (AV)-nodal blockers, aspirin and anticoagulants, and remained significant after further adjustment for inflammatory markers (2.05 (1.29 to 3.26)). Results were similar after excluding those taking AV-nodal blocker medications. There was no effect modification of these associations by sex or age.
Elevated RHR was positively associated with VTE incidence after a median of 14 years; this association was independent of several traditional VTE and inflammatory markers.
静脉血栓栓塞症(VTE)与显著的发病率和死亡率相关。静息心率(RHR)可通过生活方式改变进行调节,已被证明与心血管疾病风险以及可预测VTE发生率的炎症标志物有关。
我们研究了RHR是否也独立于这些风险因素与VTE发生率相关。我们对6479名动脉粥样硬化多民族研究参与者进行了研究,这些参与者在基线时无临床VTE,且通过12导联心电图确定了基线RHR。使用国际疾病分类(ICD)-9和ICD-10编码从医院记录和死亡证明中记录VTE事件。我们将RHR分为<60、60 - 69、70 - 79和≥80次/分钟。我们使用Cox风险模型来确定RHR与VTE发生率之间的关联。
参与者的平均(标准差)年龄为62(10)岁,RHR为63(10)次/分钟。RHR与多种炎症和凝血因子呈横断面相关。在中位随访14年后有236例VTE病例。与RHR<60次/分钟的人相比,RHR≥80次/分钟的人发生VTE的风险比(95%置信区间)为2.08(1.31至3.30),在调整了人口统计学、身体活动、吸烟、糖尿病以及使用房室(AV)结阻滞剂、阿司匹林和抗凝剂后,在进一步调整炎症标志物后仍具有显著性(2.05(1.29至3.26))。排除服用AV结阻滞剂药物的人后结果相似。这些关联在性别或年龄方面没有效应修饰。
在中位14年后,升高的RHR与VTE发生率呈正相关;这种关联独立于几种传统的VTE和炎症标志物。