Iñiguez-Ariza Nicole M, Bible Keith C, Clarke Bart L
Division of Endocrinology, Diabetes, Metabolism, and Nutrition, Mayo Clinic, 200 First Street SW Rochester, MN, 55905, USA.
Department of Endocrinology and Metabolism, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, Mexico City, Mexico.
J Bone Oncol. 2020 Feb 19;21:100282. doi: 10.1016/j.jbo.2020.100282. eCollection 2020 Apr.
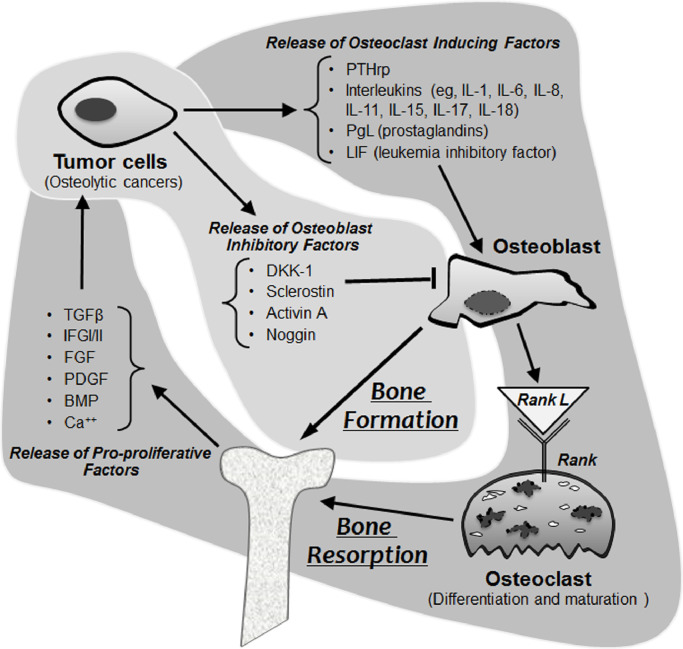
Whereas preemptive screening for the presence of lymph node and lung metastases is standard-of-care in thyroid cancer patients, bone metastases are less well studied and are often neglected in thyroid cancer patient surveillance. Bone metastases in thyroid cancer are, however, independently associated with poor/worse prognosis with a median overall survival from detection of only 4 years despite an otherwise excellent prognosis for the vast majority of thyroid cancer patients. In this review we summarize the state of current knowledge as pertinent to bony metastatic disease in thyroid cancer, including clinical implications, impacts on patient function and quality of life, pathogenesis, and therapeutic opportunities, proposing approaches to patient care accordingly. In particular, bone metastasis pathogenesis appears to reflect cooperatively between cancer and the bone microenvironment creating a "vicious cycle" of bone destruction rather than due exclusively to tumor invasion into bone. Additionally, bone metastases are more frequent in follicular and medullary thyroid cancers, requiring closer bone surveillance in patients with these histologies. Emerging data also suggest that treatments such as multikinase inhibitors (MKIs) can be less effective in controlling bone, as opposed to other (e.g. lung), metastases in thyroid cancers, making special attention to bone critical even in the setting of active MKI therapy. Although locoregional therapies including surgery, radiotherapy and ablation play important roles in palliation, antiresorptive agents including bisphosphonates and denosumab appear individually to delay and/or lessen skeletal morbidity and complications, with dosing frequency of every 3 months appearing optimal; their early application should therefore be strongly considered.
虽然对甲状腺癌患者进行淋巴结和肺转移的预防性筛查是标准治疗方法,但骨转移的研究较少,在甲状腺癌患者的监测中常常被忽视。然而,甲状腺癌的骨转移与预后不良/较差独立相关,尽管绝大多数甲状腺癌患者的预后良好,但从发现骨转移起的中位总生存期仅为4年。在本综述中,我们总结了与甲状腺癌骨转移疾病相关的当前知识状态,包括临床意义、对患者功能和生活质量的影响、发病机制和治疗机会,并相应地提出了患者护理方法。特别是,骨转移发病机制似乎反映了癌症与骨微环境之间的协同作用,形成了骨破坏的“恶性循环”,而不仅仅是由于肿瘤侵入骨骼。此外,骨转移在滤泡状和髓样甲状腺癌中更为常见,需要对这些组织学类型的患者进行更密切的骨监测。新出现的数据还表明,与甲状腺癌的其他(如肺)转移相比,多激酶抑制剂(MKIs)等治疗在控制骨转移方面可能效果较差,即使在积极的MKI治疗情况下,对骨转移的特别关注也至关重要。尽管包括手术、放疗和消融在内的局部区域治疗在缓解症状方面发挥着重要作用,但包括双膦酸盐和地诺单抗在内的抗吸收剂似乎单独使用可延迟和/或减轻骨骼发病率和并发症,每3个月给药一次似乎是最佳频率;因此,应强烈考虑早期应用。