Division of Urology, Department of Surgery, Princess Margaret Cancer Centre, University Health Network, University of Toronto, Toronto, Ontario, Canada.
Department of Urology, University Hospital of Zurich, University of Zurich, Zurich, Switzerland.
Cancer Med. 2020 May;9(10):3287-3296. doi: 10.1002/cam4.2980. Epub 2020 Mar 12.
Single-arm trials are currently an accepted study design to investigate the efficacy of novel therapies (NT) in non-muscle invasive bladder cancer (NMIBC) unresponsive to intravesical Bacillus Calmette-Guérin (BCG) immunotherapy as randomized controlled trials are either unfeasible (comparator: early radical cystectomy; ERC), or unethical (comparator: placebo). To guide the design of such single-arm trials, expert groups published recommendations for clinically meaningful outcomes. The aim of this study was to quantitatively verify the appropriateness of these recommendations.
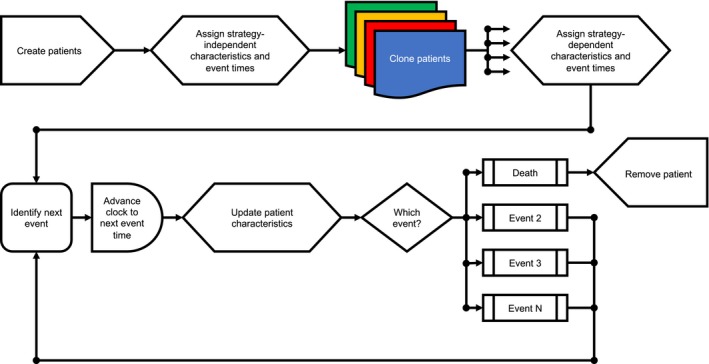
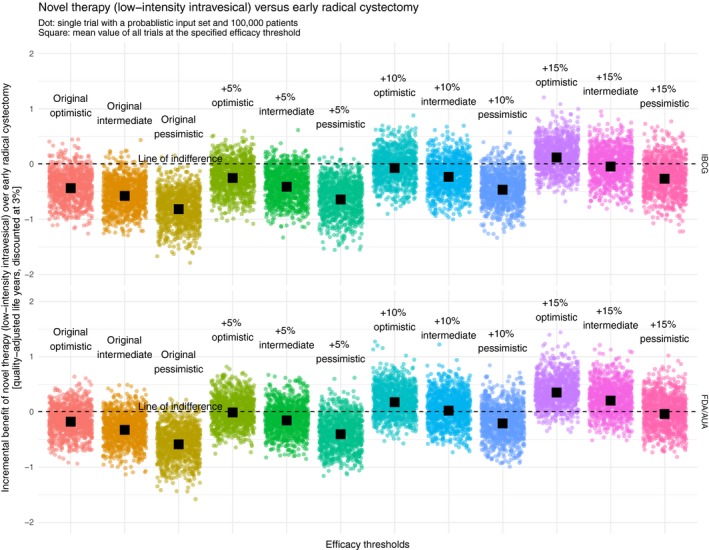
We used a discrete event simulation framework in combination with a supercomputer to find the required efficacy at which a NT can compete with ERC when it comes to quality-adjusted life expectancy (QALE). In total, 24 different efficacy thresholds (including the recommendations) were investigated.
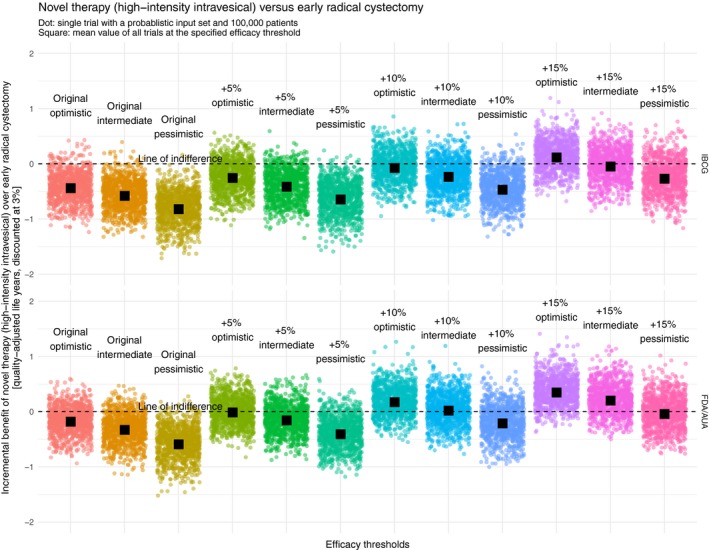
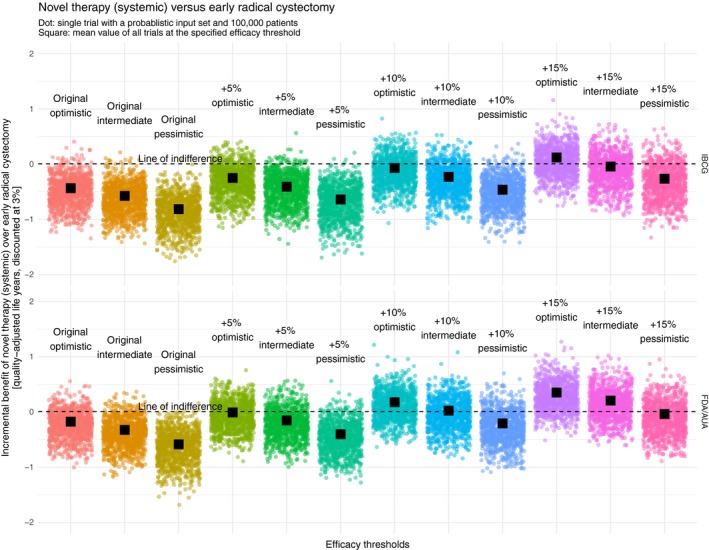
After ascertaining face validity with content experts, repeated verification, external validation, and calibration we considered our model valid. Both recommendations rarely showed an incremental benefit of the NT over ERC. In the most optimistic scenario, an increase in the IBCG recommendation by 10% and an increase in the FDA/AUA recommendation by 5% would yield results at which a NT could compete with ERC from a QALE perspective.
This simulation study demonstrated that the current recommendations regarding clinically meaningful outcomes for single-arm trials evaluating the efficacy of NT in BCG-unresponsive NMIBC may be too low. Based on our quantitative approach, we propose increasing these thresholds to at least 45%-55% at 6 months and 35% at 18-24 months (complete response rates/recurrence-free survival) to promote the development of clinically truly meaningful NT.
单臂试验目前是一种被接受的研究设计,用于研究新型疗法(NT)在对卡介苗(BCG)免疫治疗无反应的非肌肉浸润性膀胱癌(NMIBC)中的疗效,因为随机对照试验要么不可行(对照:早期根治性膀胱切除术;ERC),要么不道德(对照:安慰剂)。为了指导此类单臂试验的设计,专家组发布了关于有临床意义的结果的建议。本研究的目的是定量验证这些建议的适当性。
我们使用离散事件模拟框架结合超级计算机,以找到 NT 在质量调整生命期望(QALE)方面与 ERC 竞争所需的疗效。总共研究了 24 个不同的疗效阈值(包括建议)。
在与内容专家确定表面效度、重复验证、外部验证和校准后,我们认为我们的模型是有效的。这两个建议很少显示 NT 比 ERC 具有额外的益处。在最乐观的情况下,将 IBCG 建议提高 10%,将 FDA/AUA 建议提高 5%,将从 QALE 的角度产生 NT 可以与 ERC 竞争的结果。
这项模拟研究表明,目前关于评估 NT 在 BCG 无反应性 NMIBC 中的疗效的单臂试验中临床有意义结果的建议可能太低了。基于我们的定量方法,我们建议将这些阈值提高到至少 6 个月时 45%-55%,18-24 个月时 35%(完全缓解率/无复发生存率),以促进真正有临床意义的 NT 的发展。