Kolkhir Pavel, Bonnekoh Hanna, Kocatürk Emek, Hide Michihiro, Metz Martin, Sánchez-Borges Mario, Krause Karoline, Maurer Marcus
Dermatological Allergology, UCARE Charité, Allergie-Centrum-Charité, Department of Dermatology and Allergy, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Berlin, Germany.
Division of Immune-mediated Skin Diseases, Sechenov First Moscow State Medical University (Sechenov University), Moscow, Russian Federation.
World Allergy Organ J. 2020 Mar 5;13(3):100107. doi: 10.1016/j.waojou.2020.100107. eCollection 2020 Mar.
Urticarial vasculitis (UV) is a rare type of leukocytoclastic vasculitis characterized by long lasting urticarial skin lesions and poor response to treatment. As of yet, no clinical guidelines, diagnostic criteria, or treatment algorithms exist, and the approaches to the diagnostic workup and treatment of UV patients may differ globally. We conducted an online survey to examine how UV patients are diagnosed and treated by international specialists and to reveal the greatest challenges in managing UV patients worldwide.
Distribution of the questionnaire included an email to individuals in the World Allergy Organization (WAO) database, with no restrictions applied to the specialty, affiliation, or nationality of the participants (November 2018). The email contained a link (Internet address) to the online questionnaire. Responses were anonymous. The link to the questionnaire was further sent to the network of Urticaria Centers of Reference and Excellence (UCARE) in the Global Allergy and Asthma European Network (GALEN) as well as to the Turkish Dermatology Society and the Japanese Society of Allergology, who distributed the link to their members. In addition, the survey link was posted online in the group of the Russian Society of Allergologists and Immunologists.
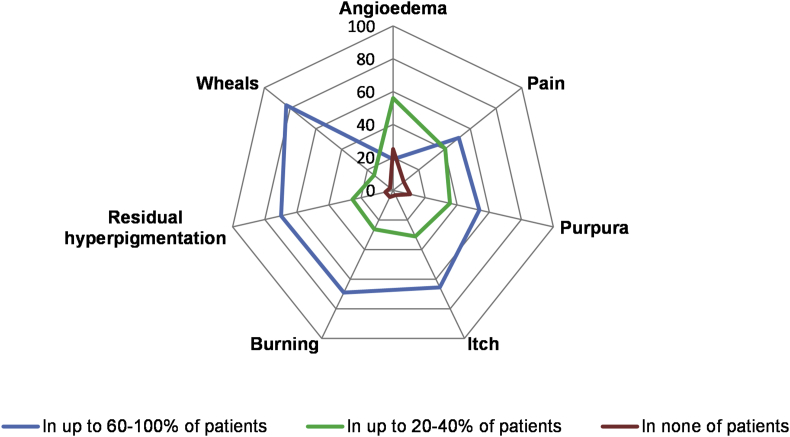
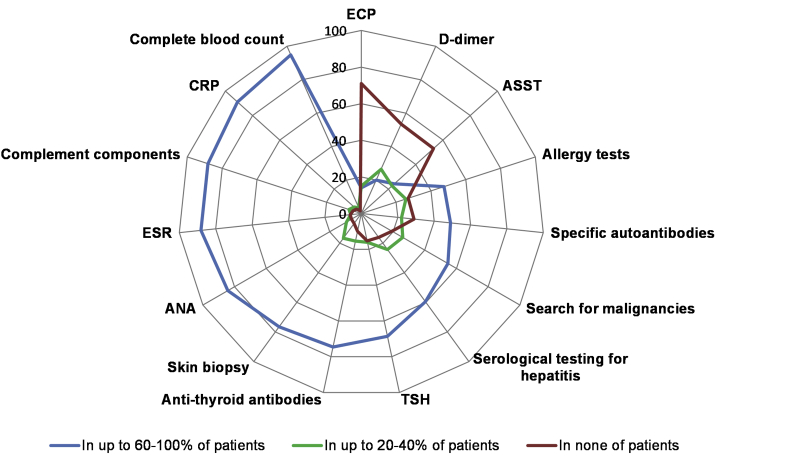
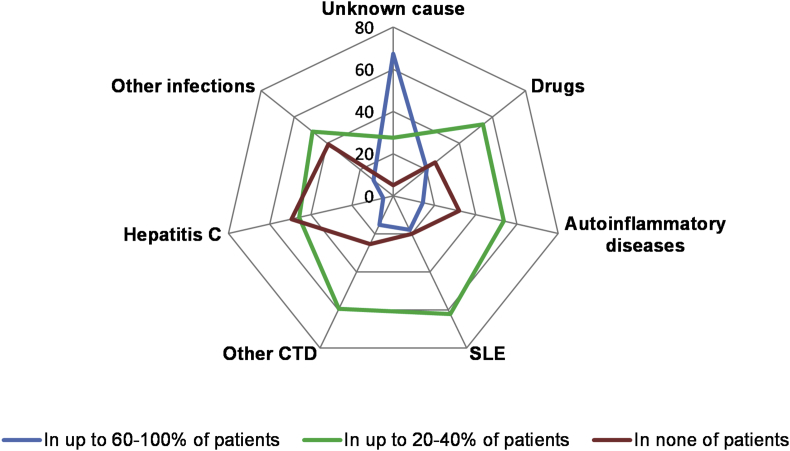
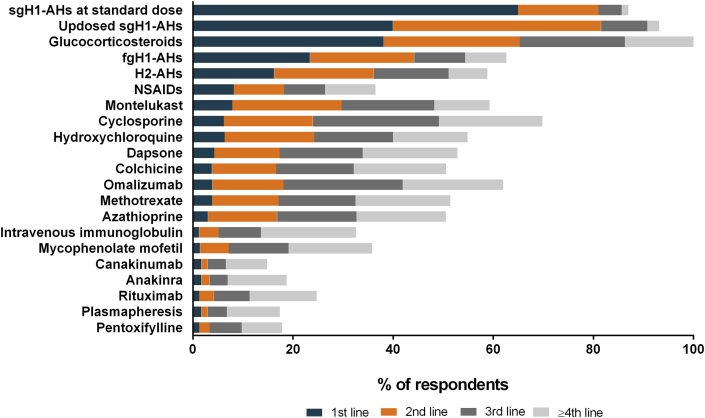
We received 883 completed surveys from physicians in 92 countries. UV was reported to be rare in clinical practice, with an average of 5 patients per physician per year. More than two-thirds of physicians reported wheals, burning of the skin, and residual hyperpigmentation in 60-100% of UV patients. The most frequently reported reason for receiving referrals of patients with UV was to establish the diagnosis. The most important features for establishing the diagnosis of UV were wheals of longer than 24 hours duration (72%), the results of skin biopsy (63%), and post-inflammatory hyperpigmentation (46%). The most common tests ordered in UV patients were complete blood count, erythrocyte sedimentation rate, C-reactive protein, complement components, antinuclear antibodies, and skin biopsy. Physicians considered UV to be of unknown cause in most patients, and drugs and systemic lupus erythematosus to be the most common identifiable causes. Two of 3 physicians reported that they use second-generation antihistamines in standard dose as the first-line therapy in patients with UV. The greatest perceived challenges in the management of UV were the limited efficacy of drugs and the absence of clinical guidelines and treatment algorithms.
UV is a challenging disease. Skin biopsy, a gold standard for UV diagnosis, is not performed by many physicians. This may lead to misdiagnosis of UV, for example, as chronic spontaneous urticaria, and to inadequate treatment. International consensus-based recommendations for the classification of UV and the diagnostic workup and treatment, as well as prospective studies evaluating potentially safe and effective drugs for the treatment of UV, are necessary.
荨麻疹性血管炎(UV)是白细胞破碎性血管炎的一种罕见类型,其特征为荨麻疹样皮肤损害持续时间长且对治疗反应不佳。迄今为止,尚无临床指南、诊断标准或治疗方案,全球范围内对UV患者的诊断检查和治疗方法可能存在差异。我们开展了一项在线调查,以了解国际专家如何诊断和治疗UV患者,并揭示全球管理UV患者面临的最大挑战。
问卷分发方式包括向世界过敏组织(WAO)数据库中的人员发送电子邮件(2018年11月),对参与者的专业、所属机构或国籍没有限制。邮件中包含在线问卷的链接(网址)。回复是匿名的。问卷链接还发送给了全球过敏和哮喘欧洲网络(GALEN)中的荨麻疹参考与卓越中心(UCARE)网络,以及土耳其皮肤病学会和日本过敏学会,它们将链接分发给各自成员。此外,调查链接还发布在俄罗斯过敏学家和免疫学家协会的群组中。
我们收到了来自92个国家医生的883份完整调查问卷。据报告,UV在临床实践中较为罕见,每位医生每年平均诊治5例患者。超过三分之二的医生报告称,60%至100%的UV患者出现风团、皮肤烧灼感和色素沉着。接收UV患者转诊的最常见原因是明确诊断。诊断UV的最重要特征是持续时间超过24小时的风团(72%)、皮肤活检结果(63%)和炎症后色素沉着(46%)。UV患者最常进行的检查是全血细胞计数、红细胞沉降率、C反应蛋白、补体成分、抗核抗体和皮肤活检。医生认为大多数UV患者病因不明,药物和系统性红斑狼疮是最常见的可识别病因。三分之二的医生报告称,他们将标准剂量的第二代抗组胺药作为UV患者的一线治疗药物。管理UV患者面临的最大挑战是药物疗效有限以及缺乏临床指南和治疗方案。
UV是一种具有挑战性的疾病。皮肤活检作为UV诊断的金标准,许多医生并未实施。这可能导致UV误诊,例如误诊为慢性自发性荨麻疹,并导致治疗不足。有必要制定基于国际共识的UV分类、诊断检查和治疗建议,以及评估治疗UV潜在安全有效药物的前瞻性研究。