Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Division of Gastroenterology and Hepatology, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Sci Rep. 2020 Mar 17;10(1):4899. doi: 10.1038/s41598-020-61874-7.
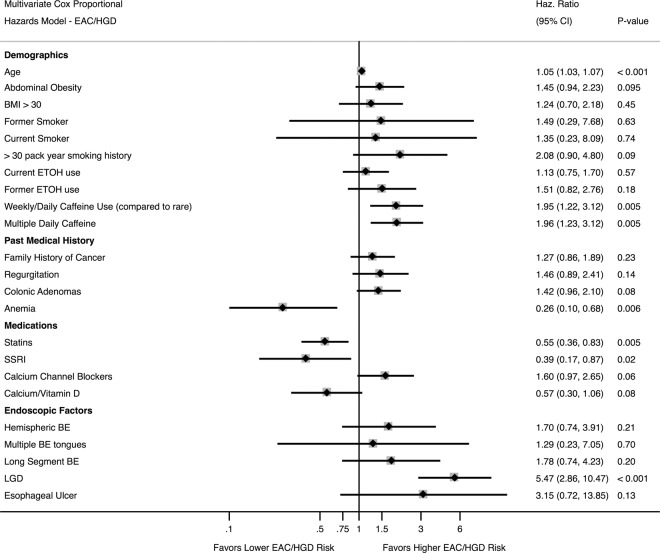
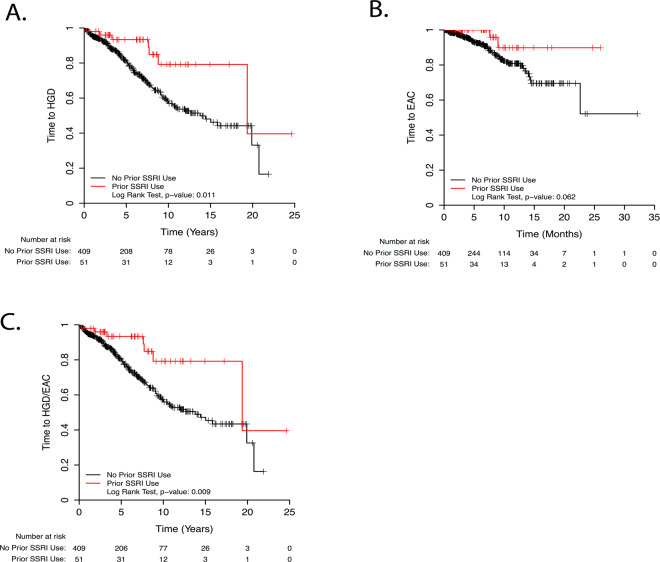
Barrett's esophagus (BE) is the only known precursor to esophageal adenocarcinoma (EAC). Methods of identifying BE patients at high risk for progression to high-grade dysplasia (HGD) or EAC are needed to improve outcomes and identify who will benefit most from intensive surveillance or ablative therapy. Clinical predictors of BE progression to HGD or EAC are poorly understood, with multiple contradictory studies. We performed a retrospective study which included 460 patients at Johns Hopkins Hospital who underwent at least 2 upper endoscopies 6 months apart showing biopsy-documented BE between 1992 and 2013. Patients with EAC or HGD at the initial endoscopy were excluded. Demographic, clinicopathological, and endoscopic data were collected. Univariate and multivariate Cox proportional hazards analyses with time to progression to HGD and EAC were performed. Among 460 patients included in the study, 132 BE patients developed HGD and 62 developed EAC. Significant EAC risk factors included age, abdominal obesity, caffeine intake, and the presence of HGD. Risk factors for HGD or EAC included age, caffeine intake, and low-grade dysplasia while colonic adenomas trended towards significance. Notably, a history of statin or SSRI usage reduced the risk of EAC or HGD by 49% or 61%, respectively. Our study validated several known and identified several novel risk factors, including a history of colonic adenomas or caffeine usage. Low-grade dysplasia was a risk factor for progression but various endoscopic characteristics were not, suggesting that screening strategies should focus on histology instead. We identified SSRIs as a new potentially chemoprotective medication.
巴雷特食管(BE)是目前已知的食管腺癌(EAC)唯一前体。需要寻找能够识别 BE 患者中进展为高级别异型增生(HGD)或 EAC 高危人群的方法,以改善预后,并确定谁将从强化监测或消融治疗中获益最大。BE 进展为 HGD 或 EAC 的临床预测因子了解甚少,多项研究结果相互矛盾。我们进行了一项回顾性研究,纳入了 1992 年至 2013 年期间在约翰霍普金斯医院接受至少 2 次间隔 6 个月以上的上消化道内镜检查且活检证实为 BE 的 460 例患者。将初次内镜检查时患有 EAC 或 HGD 的患者排除在外。收集了人口统计学、临床病理学和内镜数据。进行了单变量和多变量 Cox 比例风险分析,以评估进展为 HGD 和 EAC 的时间。在纳入的 460 例患者中,132 例 BE 患者发展为 HGD,62 例发展为 EAC。EAC 的显著危险因素包括年龄、腹部肥胖、咖啡因摄入和 HGD 的存在。HGD 或 EAC 的危险因素包括年龄、咖啡因摄入和低级别异型增生,而结肠腺瘤呈显著趋势。值得注意的是,他汀类药物或 SSRI 的使用史分别使 EAC 或 HGD 的风险降低了 49%或 61%。本研究验证了一些已知的危险因素,并确定了一些新的危险因素,包括结肠腺瘤或咖啡因摄入史。低级别异型增生是进展的危险因素,但各种内镜特征不是,这表明筛查策略应侧重于组织学而非内镜。我们确定了 SSRI 是一种新的潜在化学预防药物。