Ashburn Nicklaus P, Hendley Nella W, Angi Ryan M, Starnes Andrew B, Nelson R Darrell, McGinnis Henderson D, Winslow James E, Cline David M, Hiestand Brian C, Stopyra Jason P
Wake Forest School of Medicine, Department of Emergency Medicine, Winston-Salem, North Carolina.
West J Emerg Med. 2020 Feb 21;21(2):455-462. doi: 10.5811/westjem.2019.11.44597.
Increased out-of-hospital time is associated with worse outcomes in trauma. Sparse literature exists comparing prehospital scene and transport time management intervals between adult and pediatric trauma patients. National Emergency Medical Services guidelines recommend that trauma scene time be less than 10 minutes. The objective of this study was to examine prehospital time intervals in adult and pediatric trauma patients.
We performed a retrospective cohort study of blunt and penetrating trauma patients in a five-county region in North Carolina using prehospital records. We included patients who were transported emergency traffic directly from the scene by ground ambulance to a Level I or Level II trauma center between 2013-2018. We defined pediatric patients as those less than 16 years old. Urbanicity was controlled for using the Centers for Medicare and Medicaid's Ambulance Fee Schedule. We performed descriptive statistics and linear mixed-effects regression modeling.
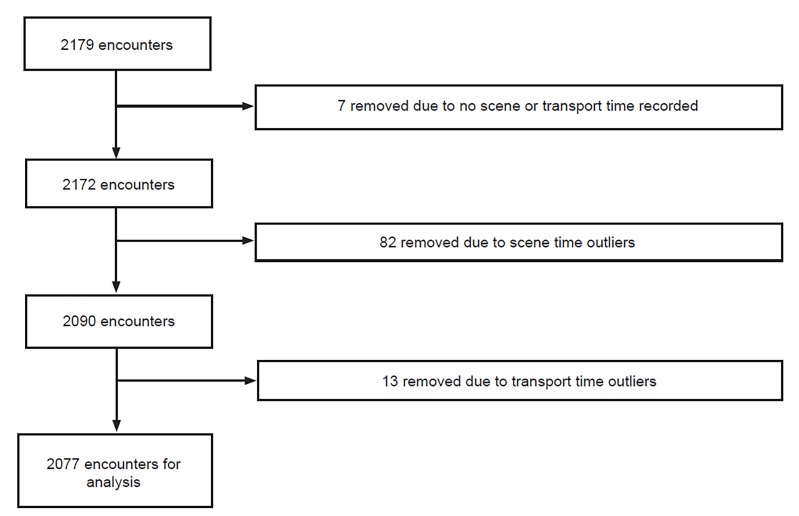
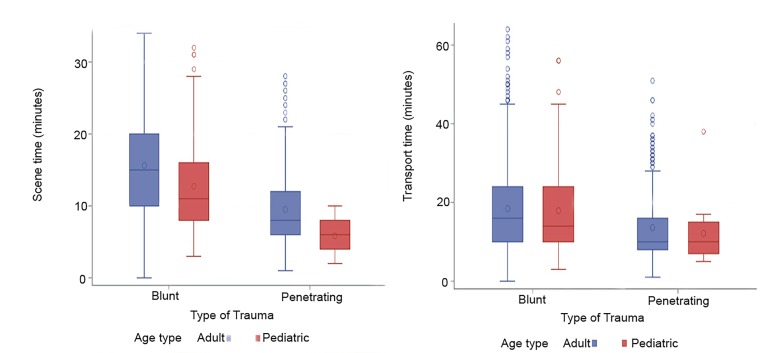
A total of 2179 records met the study criteria, of which 2077 were used in the analysis. Mean scene time was 14.2 minutes (95% confidence interval [CI], 13.9-14.5) and 35.3% (n = 733) of encounters had a scene time of 10 minutes or less. Mean transport time was 17.5 minutes (95% CI, 17.0-17.9). Linear mixed-effects regression revealed that scene times were shorter for pediatric patients (p<0.0001), males (p=0.0016), penetrating injury (p<0.0001), and patients with blunt trauma in rural settings (p=0.005), and that transport times were shorter for males (p = 0.02), non-White patients (p<0.0001), and patients in urban areas (p<0.0001).
This study population largely missed the 10-minute scene time goal. Demographic and patient factors were associated with scene and transport times. Shorter scene times occurred with pediatric patients, males, and among those with penetrating trauma. Additionally, suffering blunt trauma while in a rural environment was associated with shorter scene time. Males, non-White patients, and patients in urban environments tended to have shorter transport times. Future studies with outcomes data are needed to identify factors that prolong out-of-hospital time and to assess the impact of out-of-hospital time on patient outcomes.
院外时间延长与创伤患者的不良预后相关。比较成人和儿童创伤患者院前现场时间和转运时间管理间隔的文献较少。国家紧急医疗服务指南建议创伤现场时间应少于10分钟。本研究的目的是检查成人和儿童创伤患者的院前时间间隔。
我们使用院前记录对北卡罗来纳州一个五县地区的钝性和穿透性创伤患者进行了一项回顾性队列研究。我们纳入了2013年至2018年间通过地面救护车从现场直接紧急转运至一级或二级创伤中心的患者。我们将儿科患者定义为年龄小于16岁的患者。使用医疗保险和医疗补助中心的救护车收费表来控制城市化程度。我们进行了描述性统计和线性混合效应回归建模。
共有2179份记录符合研究标准,其中2077份用于分析。平均现场时间为14.2分钟(95%置信区间[CI],13.9 - 14.5),35.3%(n = 733)的病例现场时间为10分钟或更短。平均转运时间为17.5分钟(95% CI,17.0 - 17.9)。线性混合效应回归显示,儿科患者(p<0.0001)、男性(p = 0.0016)、穿透性损伤患者(p<0.0001)以及农村地区钝性创伤患者(p = 0.005)的现场时间较短;男性(p = 0.02)、非白人患者(p<0.0001)以及城市地区患者(p<0.0001)的转运时间较短。
本研究人群大多未达到10分钟的现场时间目标。人口统计学和患者因素与现场时间和转运时间相关。儿科患者、男性以及穿透性创伤患者的现场时间较短。此外,在农村环境中遭受钝性创伤与较短的现场时间相关。男性、非白人患者以及城市环境中的患者往往转运时间较短。需要进行有结局数据的未来研究,以确定延长院外时间的因素,并评估院外时间对患者结局的影响。