Hosein Amalia, Stoute Valerie, Chadee Samantha, Singh Natasha Ramroop
Biomedical Engineering, The University of Trinidad and Tobago, O'Meara, Arima, Trinidad & Tobago.
Environmental Studies, The University of Trinidad and Tobago, O'Meara, Arima, Trinidad & Tobago.
PeerJ. 2020 Mar 9;8:e8232. doi: 10.7717/peerj.8232. eCollection 2020.
Cardiovascular Disease (CVD) risk prediction models have been useful in estimating if individuals are at low, intermediate, or high risk, of experiencing a CVD event within some established time frame, usually 10 years. Central to this is the concern in Trinidad and Tobago of using pre-existing CVD risk prediction methods, based on populations in the developed world (e.g. ASSIGN, Framingham and QRISK2), to establish risk for its multiracial/ethnic Caribbean population. The aim of this study was to determine which pre-existing CVD risk method is best suited for predicting CVD risk for individuals in this population.
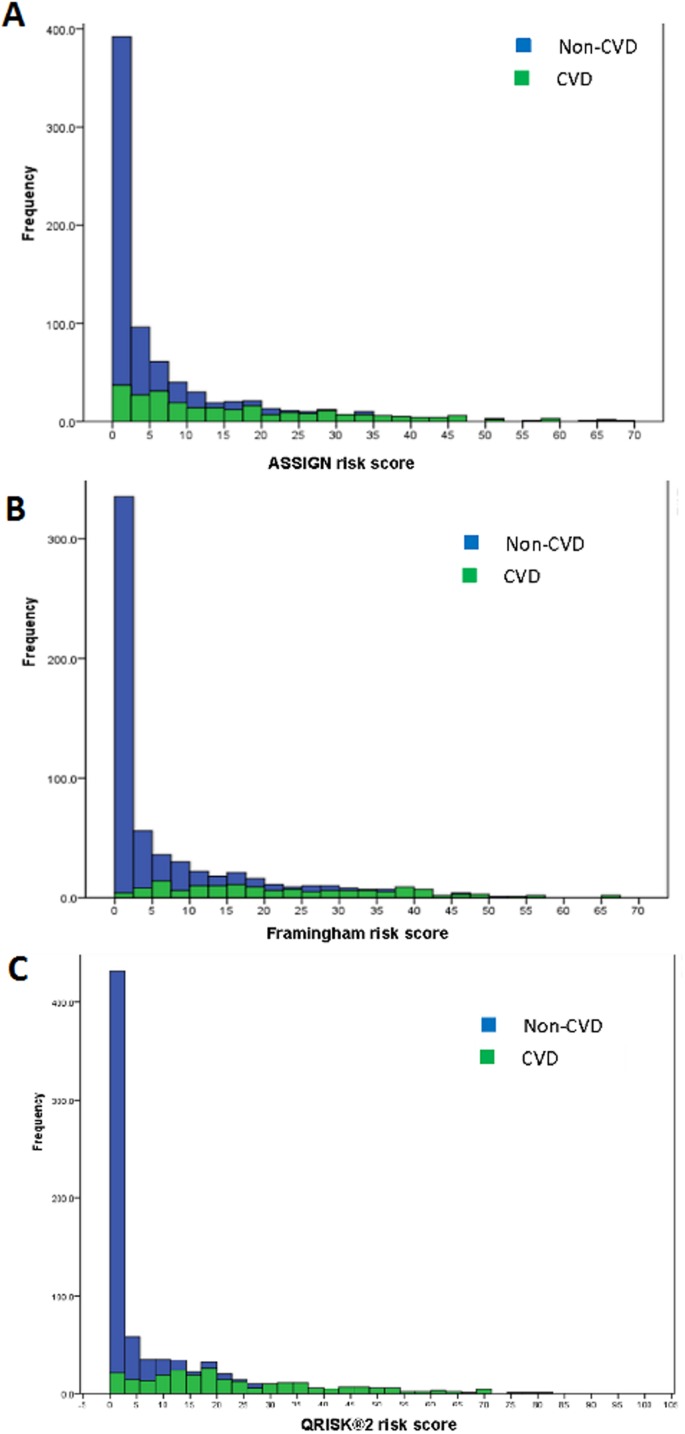
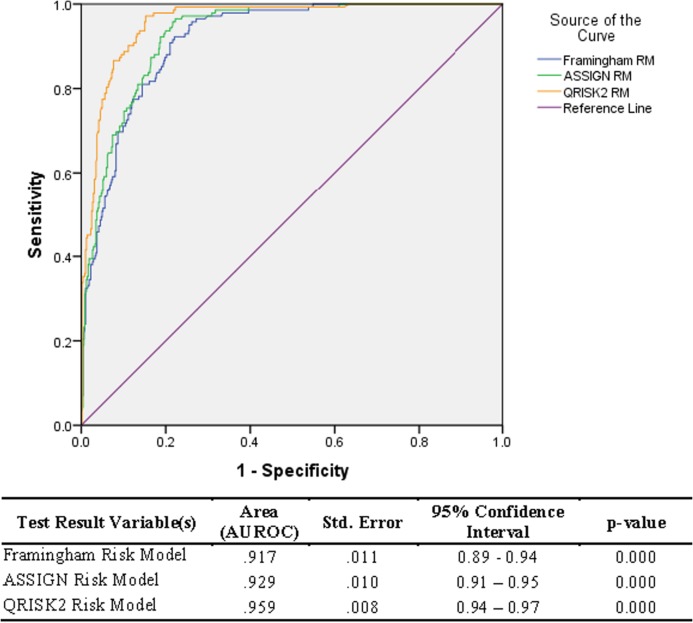
A survey was completed by 778 participants, 526 persons with no prior CVD, and 252 who previously reported a CVD event. Lifestyle and biometric data was collected from non-CVD participants, while for CVD participants, medical records were used to collect data at the first instance of CVD. The performances of three CVD risk prediction models (ASSIGN, Framingham and QRISK2) were evaluated using their calculated risk scores.
All three models (ASSIGN, Framingham and QRISK2) identified less than 62% of cases (CVD participants) with a high proportion of false-positive predictions to true predictions as can be seen by positive predictabilities ranging from 78% (ASSIGN and Framingham) to 87% (QRISK2). Further, for all three models, individuals whose scores fell into the misclassification range were 2X more likely to be individuals who had experienced a prior CVD event as opposed to healthy individuals.
The ASSIGN, Framingham and QRISK2 models should be utilised with caution on a Trinidad and Tobago population of intermediate and high risk for CVD since these models were found to have underestimated the risk for individuals with CVD up to 2.5 times more often than they overestimated the risk for healthy persons.
心血管疾病(CVD)风险预测模型有助于估计个体在既定时间段(通常为10年)内发生CVD事件的风险是低、中还是高。这其中的核心问题是,特立尼达和多巴哥担心使用基于发达国家人群(如ASSIGN、弗雷明汉和QRISK2)的现有CVD风险预测方法来确定其多民族加勒比人群的风险。本研究的目的是确定哪种现有的CVD风险方法最适合预测该人群个体的CVD风险。
778名参与者完成了一项调查,其中526人无既往CVD病史,252人曾报告有CVD事件。从无CVD的参与者中收集生活方式和生物特征数据,而对于有CVD的参与者,在CVD首次发生时使用病历收集数据。使用计算出的风险评分评估三种CVD风险预测模型(ASSIGN、弗雷明汉和QRISK2)的性能。
所有三种模型(ASSIGN、弗雷明汉和QRISK2)识别出的病例(有CVD的参与者)不到62%,假阳性预测与真阳性预测的比例很高,阳性预测值从78%(ASSIGN和弗雷明汉)到87%(QRISK2)不等。此外,对于所有三种模型,得分落入错误分类范围的个体发生过CVD事件的可能性是健康个体的两倍。
在特立尼达和多巴哥患有CVD的中高风险人群中,应谨慎使用ASSIGN、弗雷明汉和QRISK2模型,因为这些模型被发现低估CVD个体风险的频率比高估健康个体风险的频率高出2.5倍。