Saint Luke's Mid America Heart Institute Kansas City.
University of Missouri Kansas City.
J Am Heart Assoc. 2020 Apr 7;9(7):e014837. doi: 10.1161/JAHA.119.014837. Epub 2020 Mar 21.
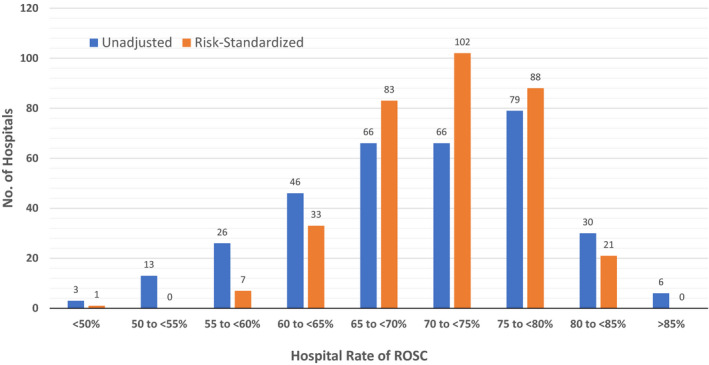
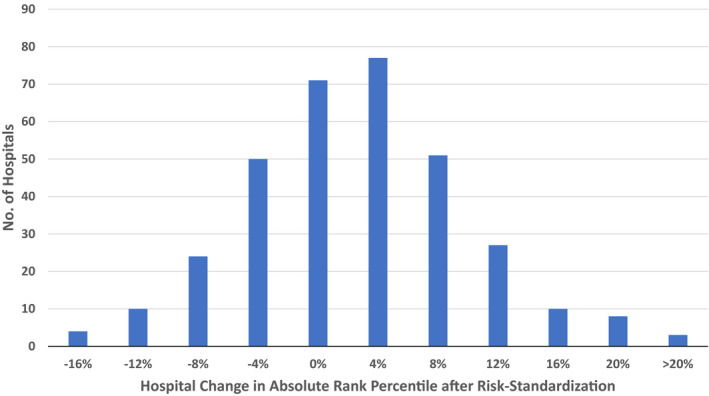
Background Sustained return of spontaneous circulation (ROSC) is the most proximal and direct assessment of acute resuscitation quality in hospitals. However, validated tools to benchmark hospital rates for ROSC after in-hospital cardiac arrest currently do not exist. Methods and Results Within the national Get With The Guidelines-Resuscitation registry, we identified 83 206 patients admitted from 335 hospitals from 2014 to 2017 with in-hospital cardiac arrest. Using hierarchical logistic regression, we derived and validated a model for ROSC, defined as spontaneous and sustained ROSC for ≥20 consecutive minutes, from 24 pre-arrest variables and calculated rates of risk-standardized ROSC for in-hospital cardiac arrest for each hospital. Overall, rates of ROSC were 72.0% and 72.7% for the derivation and validation cohorts, respectively. The model in the derivation cohort had moderate discrimination (C-statistic 0.643) and excellent calibration ( of 0.996). Seventeen variables were associated with ROSC, and a parsimonious model retained 10 variables. Before risk-adjustment, the median hospital ROSC rate was 70.5% (interquartile range: 64.7-76.9%; range: 33.3-89.6%). After adjustment, the distribution of risk-standardized ROSC rates was narrower: median of 71.9% (interquartile range: 68.2-76.4%; range: 42.2-84.6%). Overall, 56 (16.7%) of 335 hospitals had at least a 10% absolute change in percentile rank after risk standardization: 27 (8.0%) with a ≥10% negative percentile change and 29 (8.7%) with a ≥10% positive percentile change. Conclusions We have derived and validated a model to risk-standardize hospital rates of ROSC for in-hospital cardiac arrest. Use of this model can support efforts to compare acute resuscitation survival across hospitals to facilitate quality improvement.
自主循环恢复(ROSC)的持续时间是医院内急性复苏质量最直接的评估指标。然而,目前尚不存在用于基准化医院在院内心搏骤停后 ROSC 发生率的验证工具。
在全国 Get With The Guidelines-Resuscitation 注册研究中,我们从 2014 年至 2017 年期间来自 335 家医院的 83206 例院内心搏骤停患者中确定了研究对象。使用分层逻辑回归,我们从 24 个心脏骤停前变量中得出并验证了一个 ROSC 模型,该模型定义为持续 20 分钟以上的自发和持续 ROSC,并计算了每个医院的院内心搏骤停风险标准化 ROSC 发生率。总体而言,推导队列和验证队列的 ROSC 发生率分别为 72.0%和 72.7%。推导队列中的模型具有中等的区分度(C 统计量 0.643)和极好的校准度(=0.996)。17 个变量与 ROSC 相关,一个简化模型保留了 10 个变量。在风险调整之前,医院 ROSC 率的中位数为 70.5%(四分位间距:64.7-76.9%;范围:33.3-89.6%)。调整后,风险标准化 ROSC 率的分布范围变窄:中位数为 71.9%(四分位间距:68.2-76.4%;范围:42.2-84.6%)。总体而言,在风险标准化后,335 家医院中有 56 家(16.7%)的百分位排名至少有 10%的绝对变化:27 家(8.0%)的负百分位变化≥10%,29 家(8.7%)的正百分位变化≥10%。
我们已经得出并验证了一个用于风险标准化医院院内心搏骤停 ROSC 发生率的模型。该模型的使用可以支持比较医院间急性复苏存活率的努力,以促进质量改进。