Yu Chi-Chang, Kuo Wen-Lin, Shen Shih-Che, Chou Hsu-Huan, Lo Yung-Feng, Yu Ming-Chin, Chen Shin-Cheh
Department of Surgery, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Department of Surgery, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Biomed J. 2020 Feb;43(1):83-93. doi: 10.1016/j.bj.2019.07.002. Epub 2020 Feb 21.
This study aimed to identify the factors that predict distant recurrence and survival outcome after patients with primary positive hormone receptor-positive (HR+) invasive breast cancer undergo complete excision for isolated local recurrence (ILR).
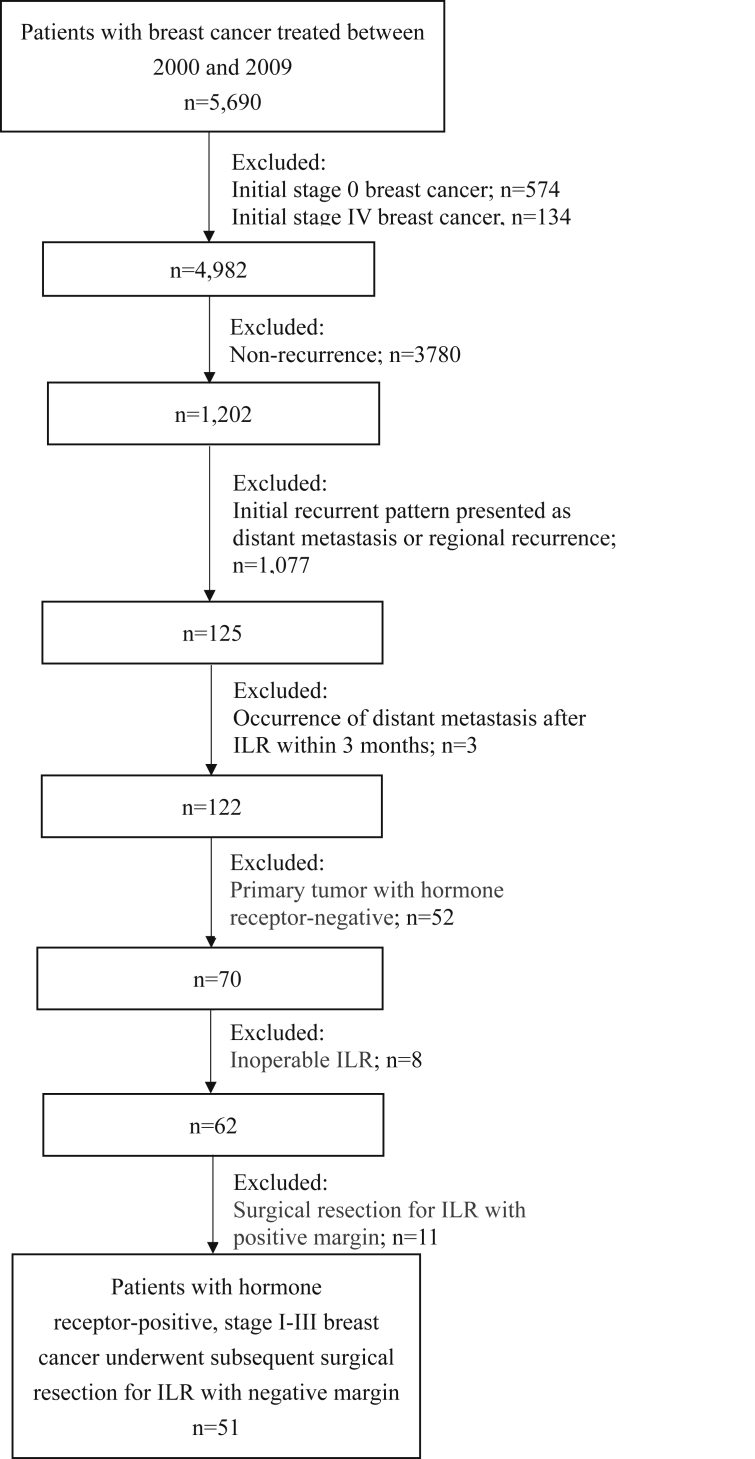
From January 2000 to December 2009, we performed a retrospective review of our database and identified 51 patients with HR + invasive breast cancer who underwent complete excision for ILR as a component of salvage therapy. The distant metastasis-free survival (DMFS) and overall survival (OS) from the time of ILR were calculated using the Kaplan-Meier method, and a Cox regression model was used for multivariate analysis.
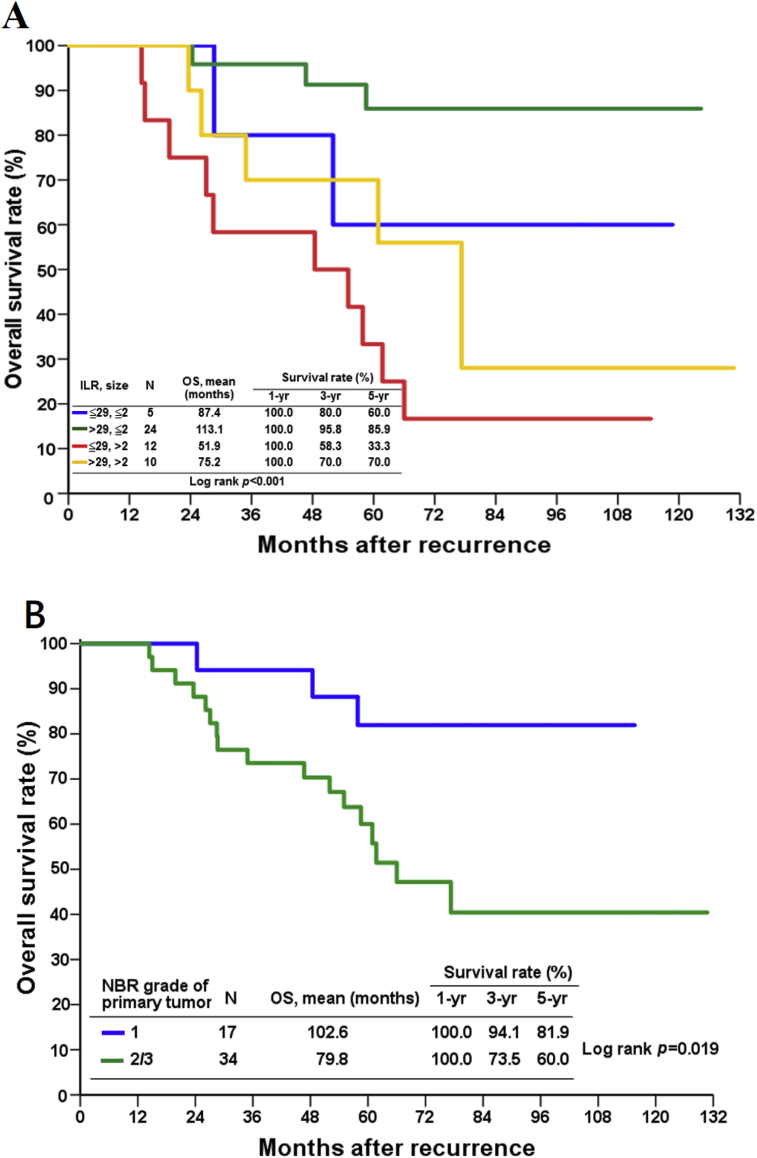
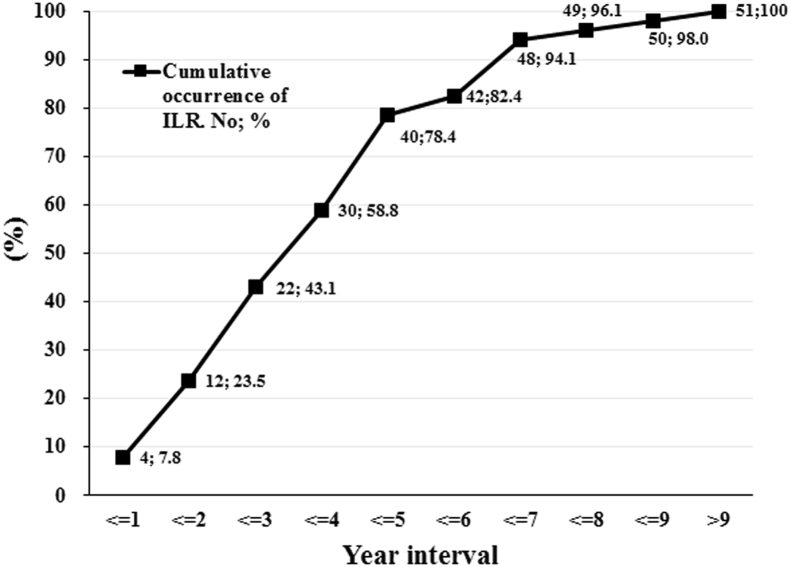
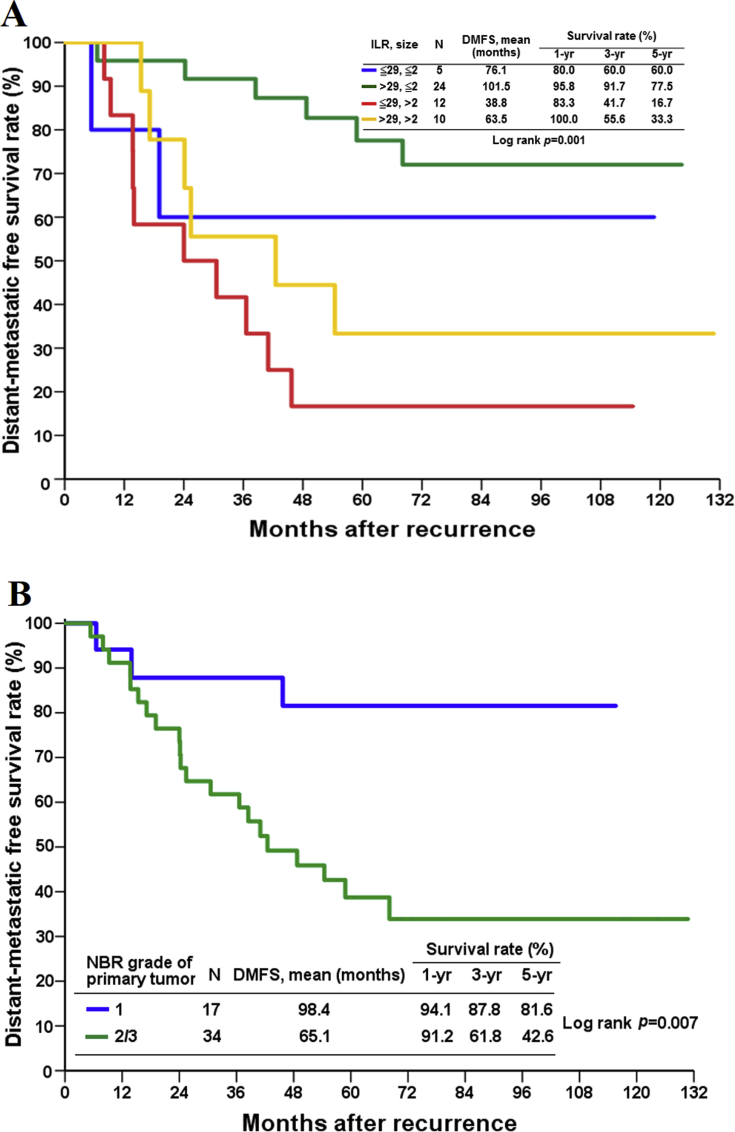
Of the 51 cases of ILR, 28 were of ipsilateral breast tumor recurrence and 23 were of chest wall recurrence. By receiver operating characteristic curve analyses, the cut-off time point for time to ILR was determined to be 29 months. According to time to ILR (≤29 vs. >29 months) and primary tumor size (≤2 vs. >2 cm), patients were divided into four risk groups as variables for analysis. On multivariate analysis, two independent prognostic factors for DMFS and OS after ILR were identified: risk groups (ILR≤29 months with primary tumor size >2 cm vs. ILR>29 months with primary tumor size ≤ 2 cm, HR = 8.53 for DMFS and HR = 11.18 for OS) and primary tumor grade (2/3 vs. 1, HR = 6.10 for DMFS and 4.27 for OS).
We demonstrated that poor DMFS and OS are associated with high risk group defined as short time to ILR (≤29 months) with primary tumor size (>2 cm) and higher primary tumor grade (2/3) among patients with HR + invasive breast cancer treated with complete excision for ILR. Therapeutic strategies for ILR based on hormone therapy with new agents should be explored in future prospective studies, especially for patients with poor outcome.
本研究旨在确定原发性激素受体阳性(HR+)浸润性乳腺癌患者因孤立性局部复发(ILR)接受完整切除术后预测远处复发和生存结局的因素。
2000年1月至2009年12月,我们对数据库进行了回顾性分析,确定了51例HR+浸润性乳腺癌患者,他们接受了完整切除ILR作为挽救性治疗的一部分。采用Kaplan-Meier法计算从ILR发生时间开始的无远处转移生存期(DMFS)和总生存期(OS),并使用Cox回归模型进行多变量分析。
在51例ILR病例中,28例为同侧乳腺肿瘤复发,23例为胸壁复发。通过受试者工作特征曲线分析,确定ILR发生时间的截断时间点为29个月。根据ILR发生时间(≤29个月与>29个月)以及原发肿瘤大小(≤2 cm与>2 cm),将患者分为四个风险组作为分析变量。多变量分析确定了ILR术后DMFS和OS的两个独立预后因素:风险组(ILR≤29个月且原发肿瘤大小>2 cm与ILR>29个月且原发肿瘤大小≤2 cm,DMFS的HR = 8.53,OS的HR = 11.18)和原发肿瘤分级(2/3级与1级,DMFS的HR = 6.10,OS的HR = 4.27)。
我们证明,在接受ILR完整切除治疗的HR+浸润性乳腺癌患者中,DMFS和OS较差与高风险组相关,高风险组定义为ILR发生时间短(≤29个月)、原发肿瘤大小(>2 cm)以及原发肿瘤分级较高(2/3级)。未来前瞻性研究应探索基于新型药物激素治疗的ILR治疗策略,尤其是对于预后较差的患者。