Kort Sharina, Brusse-Keizer Marjolein, Gerritsen Jan Willem, Schouwink Hugo, Citgez Emanuel, de Jongh Frans, van der Maten Jan, Samii Suzy, van den Bogart Marco, van der Palen Job
Dept of Pulmonary Medicine, Medisch Spectrum Twente, Enschede, the Netherlands.
Medical School Twente, Medisch Spectrum Twente, Enschede, the Netherlands.
ERJ Open Res. 2020 Mar 16;6(1). doi: 10.1183/23120541.00221-2019. eCollection 2020 Jan.
Exhaled-breath analysis of volatile organic compounds could detect lung cancer earlier, possibly leading to improved outcomes. Combining exhaled-breath data with clinical parameters may improve lung cancer diagnosis.
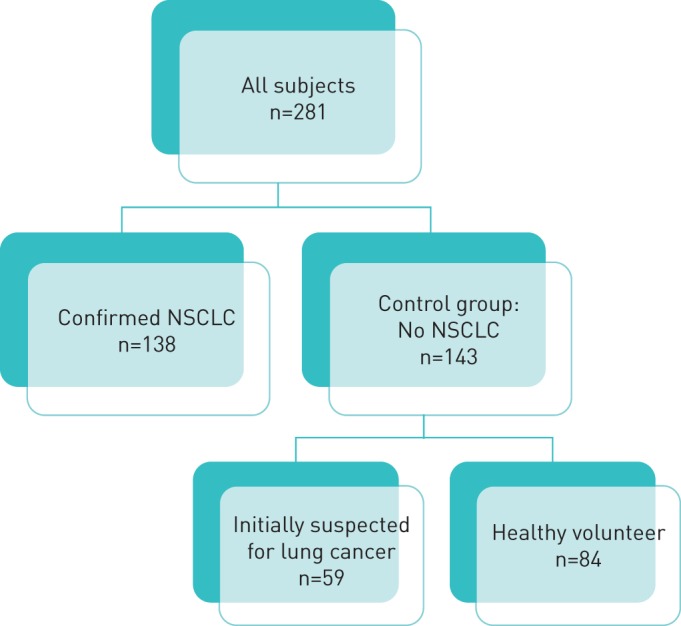
Based on data from a previous multi-centre study, this article reports additional analyses. 138 subjects with non-small cell lung cancer (NSCLC) and 143 controls without NSCLC breathed into the Aeonose. The diagnostic accuracy, presented as area under the receiver operating characteristic curve (AUC-ROC), of the Aeonose itself was compared with 1) performing a multivariate logistic regression analysis of the distinct clinical parameters obtained, and 2) using this clinical information beforehand in the training process of the artificial neural network (ANN) for the breath analysis.
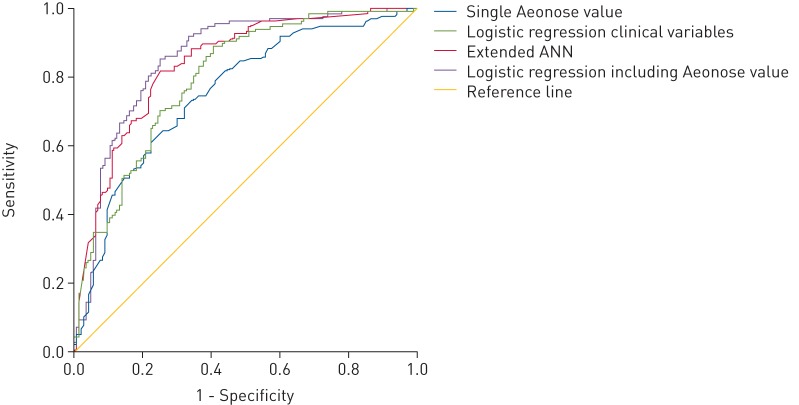
NSCLC patients (mean±sd age 67.1±9.1 years, 58% male) were compared with controls (62.1±7.0 years, 40.6% male). The AUC-ROC of the classification value of the Aeonose itself was 0.75 (95% CI 0.69-0.81). Adding age, number of pack-years and presence of COPD to this value in a multivariate regression analysis resulted in an improved performance with an AUC-ROC of 0.86 (95% CI 0.81-0.90). Adding these clinical variables beforehand to the ANN for classifying the breath print also led to an improved performance with an AUC-ROC of 0.84 (95% CI 0.79-0.89).
Adding readily available clinical information to the classification value of exhaled-breath analysis with the Aeonose, either in a multivariate regression analysis or to the ANN, significantly improves the diagnostic accuracy to detect the presence or absence of lung cancer.
对挥发性有机化合物进行呼出气分析能够更早地检测出肺癌,可能会改善治疗结果。将呼出气数据与临床参数相结合或许能提高肺癌诊断水平。
基于之前一项多中心研究的数据,本文报告了额外的分析。138名非小细胞肺癌(NSCLC)患者和143名无NSCLC的对照者向Aeonose呼气。将Aeonose本身的诊断准确性(以受试者工作特征曲线下面积(AUC-ROC)表示)与以下两种情况进行比较:1)对所获得的不同临床参数进行多因素逻辑回归分析;2)在用于呼气分析的人工神经网络(ANN)训练过程中预先使用这些临床信息。
将NSCLC患者(平均±标准差年龄67.1±9.1岁,58%为男性)与对照者(62.1±7.0岁,40.6%为男性)进行比较。Aeonose本身分类值的AUC-ROC为0.75(95%CI 0.69 - 0.81)。在多因素回归分析中,将年龄、吸烟包年数和慢性阻塞性肺疾病(COPD)的存在情况添加到该值中,性能得到改善,AUC-ROC为0.86(95%CI 0.81 - 0.90)。预先将这些临床变量添加到用于分类呼吸印记的ANN中也使性能得到改善,AUC-ROC为0.84(95%CI 0.79 - 0.89)。
在多因素回归分析中或在ANN中,将易于获得的临床信息添加到使用Aeonose进行的呼出气分析分类值中,可显著提高检测肺癌是否存在的诊断准确性。