Princess Margaret Cancer Centre, University Health Network, Toronto, ON, Canada.
Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada.
Prostate Cancer Prostatic Dis. 2020 Dec;23(4):630-637. doi: 10.1038/s41391-020-0221-7. Epub 2020 Mar 13.
Statins inhibit HMG-CoA reductase, the rate-limiting enzyme of the mevalonate pathway. Epidemiological and pre-clinical evidence support an association between statin use and delayed prostate cancer (PCa) progression. Here, we evaluated the effects of neoadjuvant fluvastatin treatment on markers of cell proliferation and apoptosis in men with localized PCa.
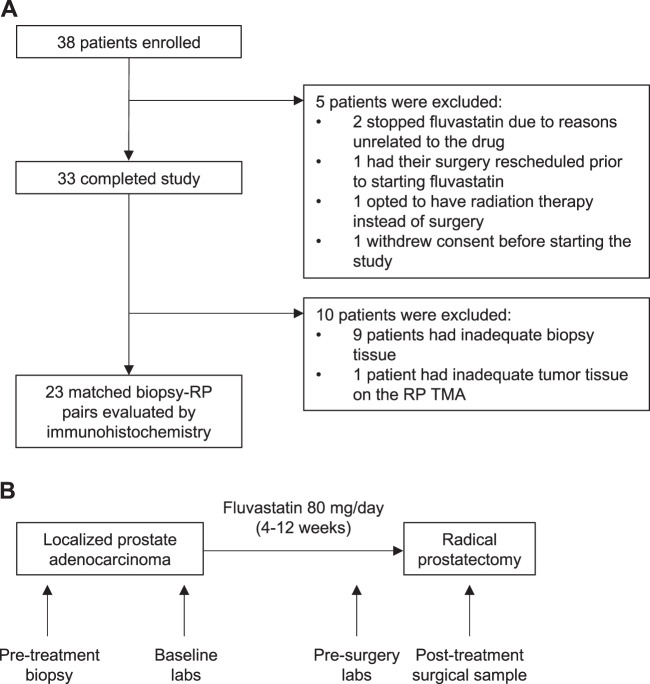
Thirty-three men were treated daily with 80 mg fluvastatin for 4-12 weeks in a single-arm window-of-opportunity study between diagnosis of localized PCa and radical prostatectomy (RP) (ClinicalTrials.gov: NCT01992042). Percent Ki67 and cleaved Caspase-3 (CC3)-positive cells in tumor tissues were evaluated in 23 patients by immunohistochemistry before and after treatment. Serum and intraprostatic fluvastatin concentrations were quantified by liquid chromatography-mass spectrometry.
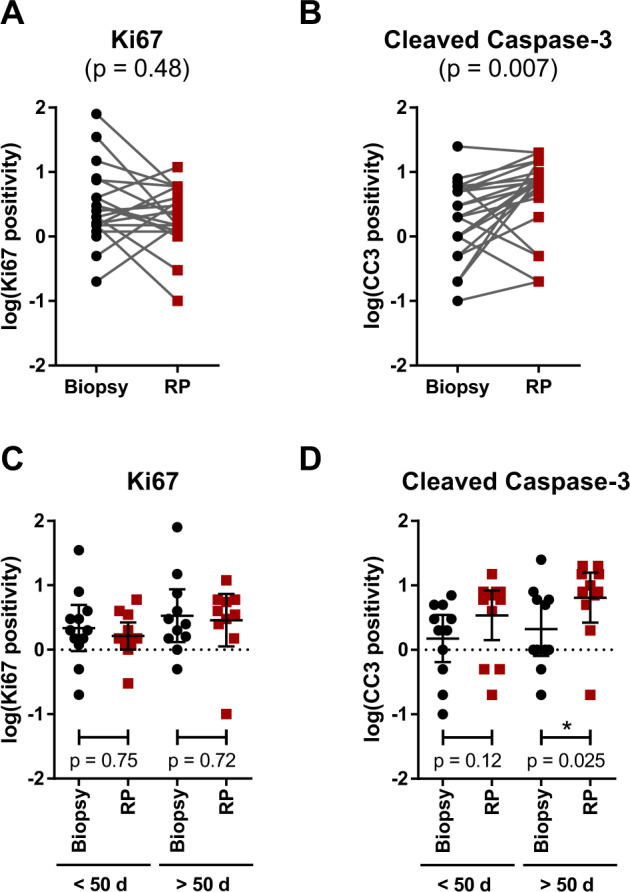
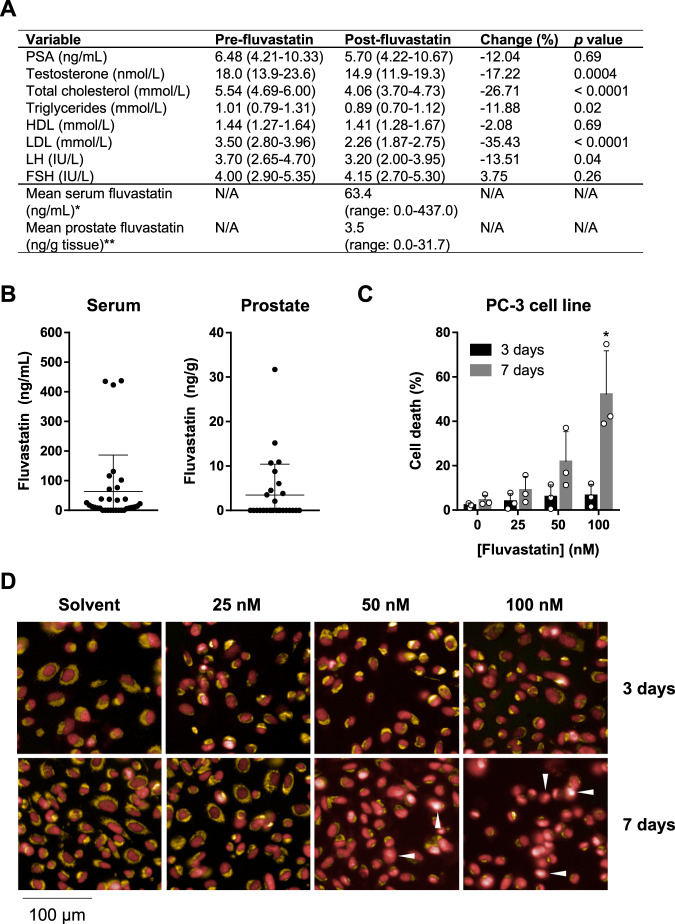
Baseline characteristics included a median prostate-specific antigen (PSA) level of 6.48 ng/mL (IQR: 4.21-10.33). The median duration of fluvastatin treatment was 49 days (range: 27-102). Median serum low-density lipoprotein levels decreased by 35% after treatment, indicating patient compliance. Median PSA decreased by 12%, but this was not statistically significant in our small cohort. The mean fluvastatin concentration measured in the serum was 0.2 μM (range: 0.0-1.1 μM), and in prostatic tissue was 8.5 nM (range: 0.0-77.0 nM). At these concentrations, fluvastatin induced PCa cell death in vitro in a dose- and time-dependent manner. In patients, fluvastatin treatment did not significantly alter intratumoral Ki67 positivity; however, a median 2.7-fold increase in CC3 positivity (95% CI: 1.9-5.0, p = 0.007) was observed in post-fluvastatin RP tissues compared with matched pre-treatment biopsy controls. In a subset analysis, this increase in CC3 was more pronounced in men on fluvastatin for >50 days.
Fluvastatin prior to RP achieves measurable drug concentrations in prostatic tissue and is associated with promising effects on tumor cell apoptosis. These data warrant further investigation into the anti-neoplastic effects of statins in prostate tissue.
他汀类药物抑制 HMG-CoA 还原酶,即甲羟戊酸途径的限速酶。流行病学和临床前证据支持他汀类药物的使用与前列腺癌(PCa)进展的延迟之间存在关联。在此,我们评估了新辅助性氟伐他汀治疗对局部 PCa 男性的细胞增殖和凋亡标志物的影响。
33 名男性在局部 PCa 诊断与根治性前列腺切除术(RP)之间,采用单臂机会窗研究,每日接受 80mg 氟伐他汀治疗 4-12 周(ClinicalTrials.gov:NCT01992042)。在治疗前后,通过免疫组织化学方法评估 23 名患者肿瘤组织中的 Ki67 和 cleaved Caspase-3(CC3)阳性细胞的百分比。通过液相色谱-质谱法定量血清和前列腺内氟伐他汀浓度。
基线特征包括中位前列腺特异性抗原(PSA)水平为 6.48ng/mL(IQR:4.21-10.33)。氟伐他汀治疗的中位持续时间为 49 天(范围:27-102)。治疗后,中位血清低密度脂蛋白水平降低 35%,表明患者依从性良好。中位 PSA 降低了 12%,但在我们的小队列中这并不具有统计学意义。在血清中测量的氟伐他汀平均浓度为 0.2μM(范围:0.0-1.1μM),在前列腺组织中为 8.5nM(范围:0.0-77.0nM)。在这些浓度下,氟伐他汀在体外以剂量和时间依赖的方式诱导 PCa 细胞死亡。在患者中,氟伐他汀治疗并未显著改变肿瘤内 Ki67 阳性率;然而,与匹配的治疗前活检对照相比,氟伐他汀治疗后 RP 组织中 CC3 阳性率中位数增加了 2.7 倍(95%CI:1.9-5.0,p=0.007)。在亚组分析中,氟伐他汀治疗超过 50 天的男性中 CC3 的增加更为明显。
RP 前氟伐他汀在前列腺组织中达到可测量的药物浓度,并与肿瘤细胞凋亡的良好效果相关。这些数据证明了他汀类药物在前列腺组织中的抗肿瘤作用值得进一步研究。