Department of Microbiology and Center of Infectious Diseases, School of Basic Medical Sciences, Peking University Health Science Center, Beijing 100191, China.
Department of Liver Disease, No. 88 Hospital of Chinese People's Liberation Army, Tai'an 271000, Shandong Province, China.
World J Gastroenterol. 2020 Mar 14;26(10):1067-1079. doi: 10.3748/wjg.v26.i10.1067.
Hepatitis B virus (HBV) infection is the primary cause of hepatitis with chronic HBV infection, which may develop into liver fibrosis, cirrhosis and hepatocellular carcinoma. Detection of early-stage fibrosis related to HBV infection is of great clinical significance to block the progression of liver lesion. Direct liver biopsy is regarded as the gold standard to detect and assess fibrosis; however, this method is invasive and prone to clinical sampling error. In order to address these issues, we attempted to find more convenient and effective serum markers for detecting HBV-induced early-stage liver fibrosis.
To investigate serum N-glycan profiling related to HBV-induced liver fibrosis and verify multiparameter diagnostic models related to serum N-glycan changes.
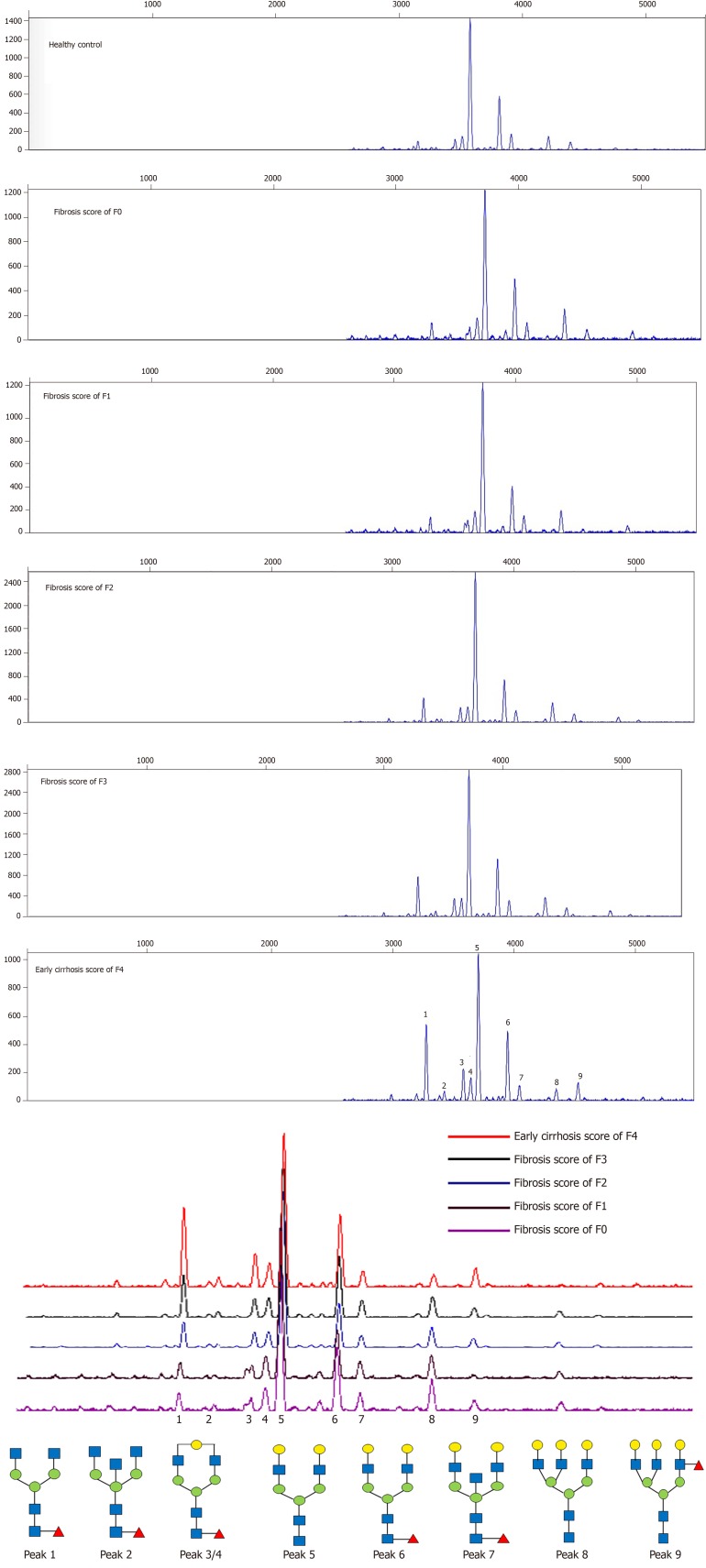
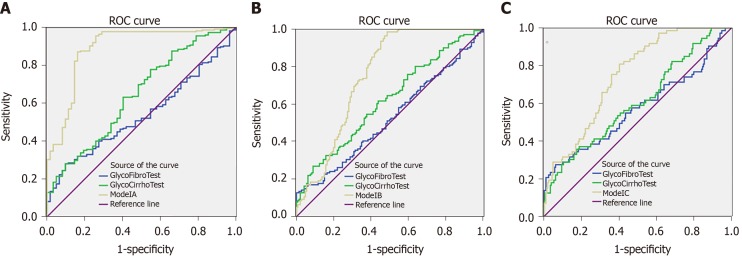
N-glycan profiles from the sera of 432 HBV-infected patients with liver fibrosis were analyzed. Significant changed N-glycan levels (peaks) ( < 0.05) in different fibrosis stages were selected in the modeling group, and multiparameter diagnostic models were established based on changed N-glycan levels by logistic regression analysis. The receiver operating characteristic (ROC) curve analysis was performed to evaluate diagnostic efficacy of N-glycans models. These models were then compared with the aspartate aminotransferase to platelet ratio index (APRI) , fibrosis index based on the four factors (FIB-4), glutamyltranspeptidase platelet albumin index (S index), GlycoCirrho-test, and GlycoFibro-test. Furthermore, we combined multiparameter diagnostic models with alanine aminotransferase (ALT) and platelet (PLT) tests and compared their diagnostic power. In addition, the diagnostic accuracy of N-glycan models was also verified in the validation group of patients.
Multiparameter diagnostic models constructed based on N-glycan peak 1, 3, 4 and 8 could distinguish between different stages of liver fibrosis. The area under ROC curves (AUROCs) of Model A and Model B were 0.890 and 0.752, respectively differentiating fibrosis F0-F1 from F2-F4, and F0-F2 from F3-F4, and surpassing other serum panels. However, AUROC (0.747) in Model C used for the diagnosis of F4 from F0-F3 was lower than AUROC (0.795) in FIB-4. In combination with ALT and PLT, the multiparameter models showed better diagnostic power (AUROC = 0.912, 0.829, 0.885, respectively) when compared with other models. In the validation group, the AUROCs of the three combined models (0.929, 0.858, and 0.867, respectively) were still satisfactory. We also applied the combined models to distinguish adjacent fibrosis stages of 432 patients (F0-F1/F2/F3/F4), and the AUROCs were 0.917, 0.720 and 0.785.
Multiparameter models based on serum N-glycans are effective supplementary markers to distinguish between adjacent fibrosis stages of patients caused by HBV, especially in combination with ALT and PLT.
乙型肝炎病毒(HBV)感染是导致肝炎的主要原因,慢性 HBV 感染可能发展为肝纤维化、肝硬化和肝细胞癌。检测与 HBV 感染相关的早期纤维化对阻止肝病变进展具有重要的临床意义。直接肝活检被认为是检测和评估纤维化的金标准;然而,这种方法具有侵入性,容易出现临床采样误差。为了解决这些问题,我们试图寻找更方便、更有效的用于检测 HBV 诱导的早期肝纤维化的血清标志物。
研究与乙型肝炎病毒诱导的肝纤维化相关的血清 N-糖组学特征,并验证与血清 N-糖变化相关的多参数诊断模型。
分析了 432 例乙型肝炎病毒感染伴肝纤维化患者血清中的 N-糖谱。在建模组中选择不同纤维化阶段(<0.05)中显著变化的 N-糖水平(峰),并通过逻辑回归分析基于变化的 N-糖水平建立多参数诊断模型。通过接受者操作特征(ROC)曲线分析评估 N-糖模型的诊断效果。然后将这些模型与天门冬氨酸氨基转移酶与血小板比值指数(APRI)、基于四个因素的纤维化指数(FIB-4)、谷氨酰转肽酶血小板白蛋白指数(S 指数)、GlycoCirrho-test 和 GlycoFibro-test 进行比较。此外,我们将多参数诊断模型与丙氨酸氨基转移酶(ALT)和血小板(PLT)检测相结合,并比较了它们的诊断能力。另外,还在验证组患者中验证了 N-糖模型的诊断准确性。
基于 N-糖峰 1、3、4 和 8 构建的多参数诊断模型能够区分不同阶段的肝纤维化。模型 A 和模型 B 的 ROC 曲线下面积(AUROCs)分别为 0.890 和 0.752,可分别区分纤维化 F0-F1 与 F2-F4,以及 F0-F2 与 F3-F4,优于其他血清标志物。然而,用于诊断 F4 与 F0-F3 的模型 C 的 AUROC(0.747)低于 FIB-4 的 AUROC(0.795)。与 ALT 和 PLT 相结合,多参数模型的诊断效能(AUROC 分别为 0.912、0.829、0.885)优于其他模型。在验证组中,三个联合模型的 AUROCs(分别为 0.929、0.858 和 0.867)仍然令人满意。我们还将联合模型应用于区分 432 例患者的相邻纤维化阶段(F0-F1/F2/F3/F4),AUROCs 分别为 0.917、0.720 和 0.785。
基于血清 N-糖的多参数模型是区分乙型肝炎病毒引起的患者相邻纤维化阶段的有效补充标志物,尤其是与 ALT 和 PLT 结合时。