Diers J, Wagner J, Baum P, Lichthardt S, Kastner C, Matthes N, Matthes H, Germer C-T, Löb S, Wiegering A
Department of General, Visceral, Transplant, Vascular and Paediatric Surgery, University Hospital, University of Würzburg, Würzburg, Germany.
Gemeinschaftskrankenhaus Havelhöhe, Berlin, Germany.
BJS Open. 2020 Apr;4(2):310-319. doi: 10.1002/bjs5.50254. Epub 2020 Jan 10.
The impact of hospital volume after rectal cancer surgery is seldom investigated. This study aimed to analyse the impact of annual rectal cancer surgery cases per hospital on postoperative mortality and failure to rescue.
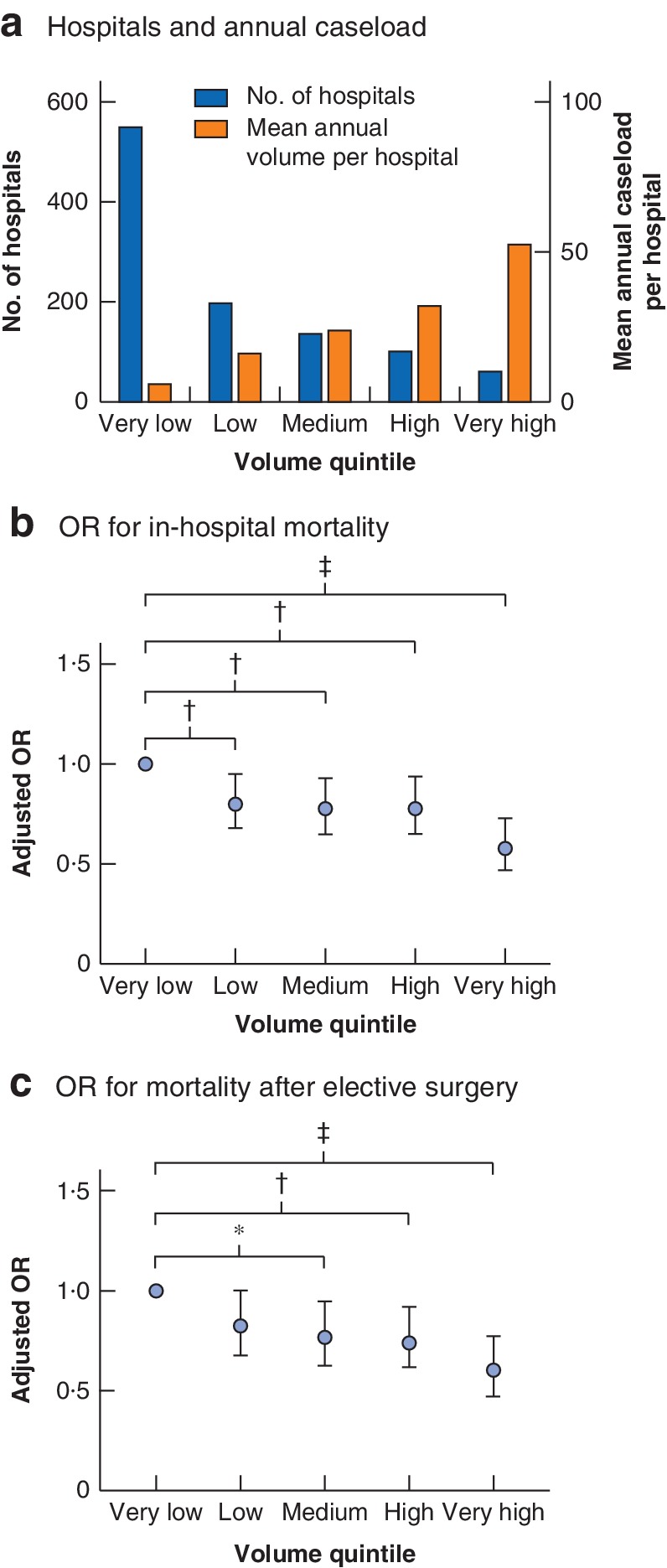
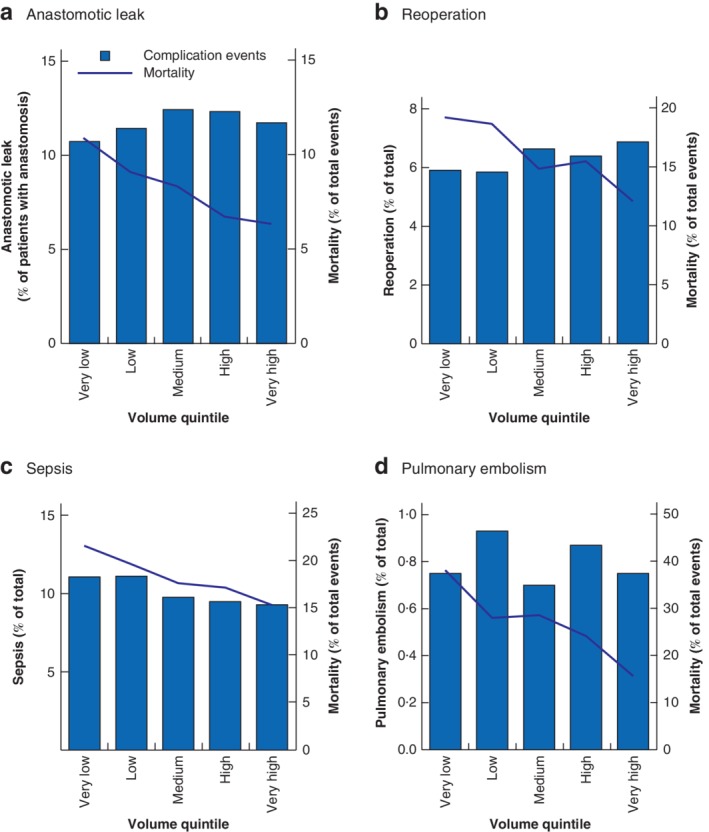
All patients diagnosed with rectal cancer and who had a rectal resection procedure code from 2012 to 2015 were identified from nationwide administrative hospital data. Hospitals were grouped into five quintiles according to caseload. The absolute number of patients, postoperative deaths and failure to rescue (defined as in-hospital mortality after a documented postoperative complication) for severe postoperative complications were determined.
Some 64 349 patients were identified. The overall in-house mortality rate was 3·9 per cent. The crude in-hospital mortality rate ranged from 5·3 per cent in very low-volume hospitals to 2·6 per cent in very high-volume centres, with a distinct trend between volume categories (P < 0·001). In multivariable logistic regression analysis using hospital volume as random effect, very high-volume hospitals (53 interventions/year) had a risk-adjusted odds ratio of 0·58 (95 per cent c.i. 0·47 to 0·73), compared with the baseline in-house mortality rate in very low-volume hospitals (6 interventions per year) (P < 0·001). The overall postoperative complication rate was comparable between different volume quintiles, but failure to rescue decreased significantly with increasing caseload (15·6 per cent after pulmonary embolism in the highest volume quintile versus 38 per cent in the lowest quintile; P = 0·010).
Patients who had rectal cancer surgery in high-volume hospitals showed better outcomes and reduced failure to rescue rates for severe complications than those treated in low-volume hospitals.
很少有研究探讨直肠癌手术后医院手术量的影响。本研究旨在分析每家医院每年的直肠癌手术病例数对术后死亡率和抢救失败率的影响。
从全国医院行政数据中识别出2012年至2015年所有诊断为直肠癌且有直肠切除手术编码的患者。根据病例数将医院分为五个五分位数组。确定了患者的绝对数量、术后死亡人数以及严重术后并发症的抢救失败率(定义为术后并发症记录后的院内死亡率)。
共识别出约64349例患者。总体院内死亡率为3.9%。粗院内死亡率从极低手术量医院的5.3%到极高手术量中心的2.6%不等,不同手术量类别之间存在明显趋势(P<0.001)。在以医院手术量为随机效应的多变量逻辑回归分析中,与极低手术量医院(每年6例手术)的基线院内死亡率相比,极高手术量医院(每年53例手术)的风险调整比值比为0.58(95%置信区间0.47至0.73)(P<0.001)。不同手术量五分位数组之间的总体术后并发症发生率相当,但随着病例数增加,抢救失败率显著降低(最高手术量五分位数组肺栓塞后为15.6%,最低五分位数组为38%;P=0.010)。
与在低手术量医院接受治疗的患者相比,在高手术量医院接受直肠癌手术的患者预后更好,严重并发症的抢救失败率更低。