Division of Health Sciences, Warwick Medical School, University of Warwick, Coventry, CV4 7AL, UK.
Institute of Applied Health Research, University of Birmingham, Birmingham, B15 2TT, UK.
BMC Gastroenterol. 2020 Mar 25;20(1):78. doi: 10.1186/s12876-020-01206-1.
The database used for the NHS Bowel Cancer Screening Programme (BCSP) derives participant information from primary care records. Combining predictors with FOBTs has shown to improve referral decisions and accuracy. The richer data available from GP databases could be used to complement screening referral decisions by identifying those at greatest risk of colorectal cancer. We determined the availability of data for key predictors and whether this information could be used to inform more accurate screening referral decisions.
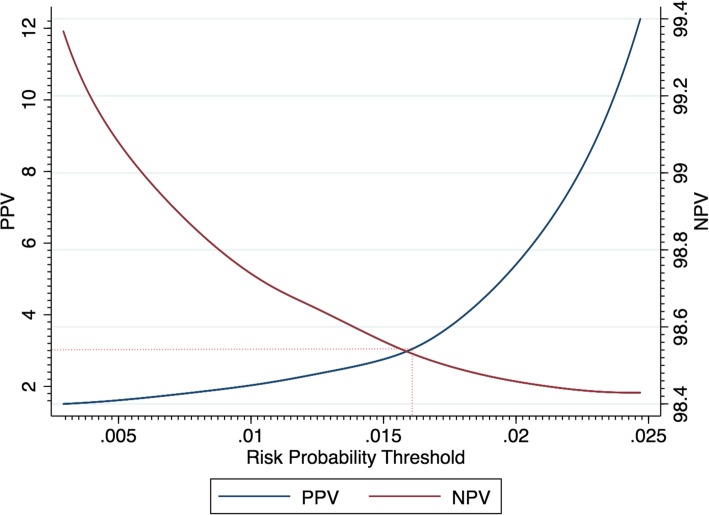
An English BCSP cohort was derived using the electronic notifications received from the BCSP database to GP records. The cohort covered a period between 13th May 2009 to 17th January 2017. Completeness of variables and univariable associations were assessed. Risk prediction models were developed using Cox regression and multivariable fractional polynomials with backwards elimination. Optimism adjusted performance metrics were reported. The sensitivity and specificity of a combined approach using the negative FOBT model plus FOBT positive patients was determined using a probability equivalent to a 3% PPV NICE guidelines level.
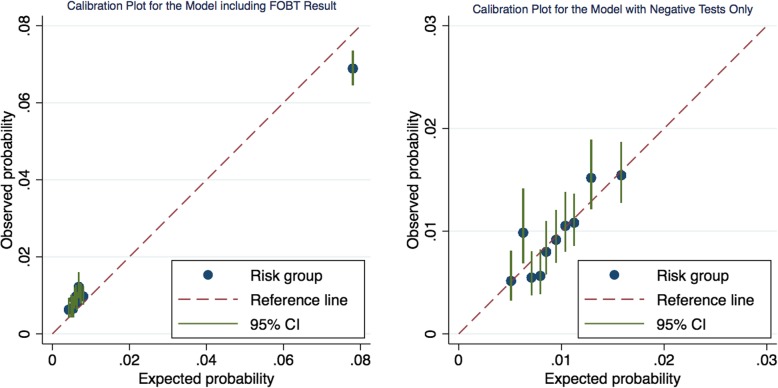
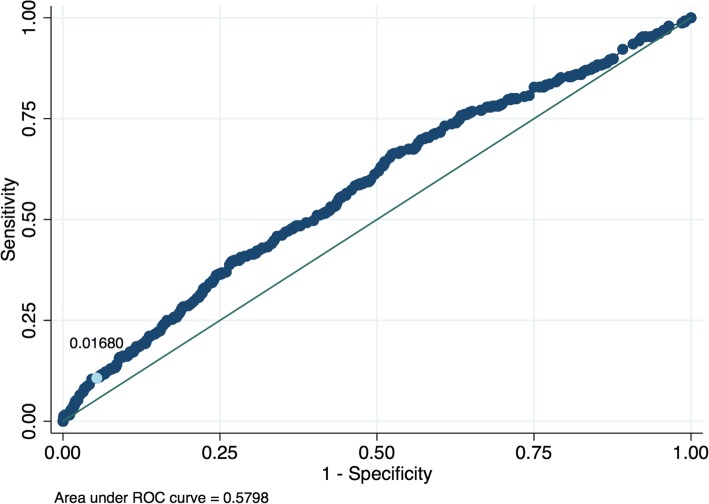
292,059 participants aged 60-74 were derived for the BCSP screening cohort. A model including the screening test result had a C-statistic of 0.860, c-slope of 0.997, and R of 0.597. A model developed for negative screening results only had a C-statistic of 0.597, c-slope of 0.940, and R of 0.062. Risk predictors included in the models included; age, sex, alcohol consumption, IBS diagnosis, family history of gastrointestinal cancer, smoking status, previous negatives and whether a GP had ordered a blood test. For the combined screening approach, sensitivity increased slightly from 53.90% (FOBT only) to 58.82% but at the expense of an increased referral rate.
This research has identified several potential predictors for CRC in a BCSP population. A risk prediction model developed for BCSP FOBT negative patients was not clinically useful due to a low sensitivity and increased referral rate. The predictors identified in this study should be investigated in a refined algorithm combining the quantitative FIT result. Combining data from multiple sources enables fuller patient profiles using the primary care and screening database interface.
英国国民保健制度(NHS)肠癌筛查计划(BCSP)使用的数据库源自初级保健记录中的参与者信息。将预测因素与粪便潜血试验(FOBT)相结合已被证明可以改善转诊决策和准确性。GP 数据库中提供的更丰富的数据可用于通过识别结直肠癌风险最大的人群来补充筛查转诊决策。我们确定了关键预测因素的数据可用性,以及这些信息是否可用于做出更准确的筛查转诊决策。
使用从 BCSP 数据库发送至 GP 记录的电子通知,在英格兰创建了一个 BCSP 队列。该队列涵盖了 2009 年 5 月 13 日至 2017 年 1 月 17 日期间的内容。评估了变量的完整性和单变量关联。使用 Cox 回归和向后消除的多变量分数多项式建立了风险预测模型。报告了经过乐观调整的性能指标。使用与 NICE 指南 3%阳性预测值(PPV)水平相当的概率确定了使用阴性 FOBT 模型加 FOBT 阳性患者的联合方法的灵敏度和特异性。
从 BCSP 筛查队列中获得了 292,059 名年龄在 60-74 岁的参与者。包含筛查测试结果的模型的 C 统计量为 0.860,c-斜率为 0.997,R 为 0.597。仅为阴性筛查结果开发的模型的 C 统计量为 0.597,c-斜率为 0.940,R 为 0.062。纳入模型的风险预测因素包括:年龄、性别、饮酒量、IBS 诊断、胃肠道癌症家族史、吸烟状况、既往阴性结果以及 GP 是否进行了血液检查。对于联合筛查方法,灵敏度从仅使用 FOBT 的 53.90%略有增加至 58.82%,但转诊率也有所增加。
本研究在 BCSP 人群中确定了几个结直肠癌的潜在预测因素。为 BCSP FOBT 阴性患者开发的风险预测模型由于灵敏度低和转诊率增加而没有临床意义。应在结合定量 FIT 结果的细化算法中进一步研究本研究中确定的预测因素。从多个来源合并数据可以使用初级保健和筛查数据库接口来构建更完整的患者资料。