Department of General and Interventional Cardiology, University Heart and Vascular Center Hamburg, Hamburg, Germany.
DZHK (German Center for Cardiovascular Research), Partner site, Hamburg/Kiel/Lübeck, Germany.
Clin Res Cardiol. 2020 Nov;109(11):1352-1357. doi: 10.1007/s00392-020-01631-y. Epub 2020 Mar 25.
Iron deficiency is now accepted as an independent entity beyond anemia. Recently, a new functional definition of iron deficiency was proposed and proved strong efficacy in randomized cardiovascular clinical trials of intravenous iron supplementation. Here, we characterize the impact of iron deficiency on all-cause mortality in the non-anemic general population based on two distinct definitions.
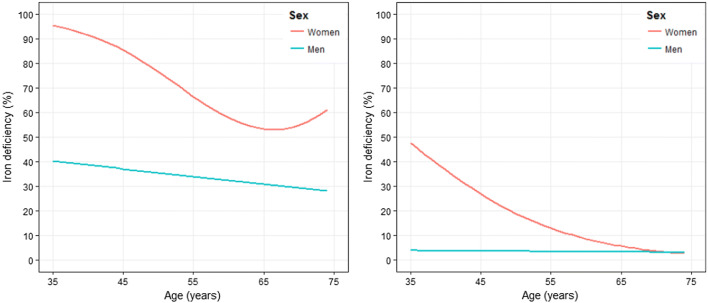
The Gutenberg Health Study is a population-based, prospective, single-center cohort study. The 5000 individuals between 35 and 74 years underwent baseline and a planned follow-up visit at year 5. Tested definitions of iron deficiency were (1) functional iron deficiency-ferritin levels below 100 µg/l, or ferritin levels between 100 and 299 µg/l and transferrin saturation below 20%, and (2) absolute iron deficiency-ferritin below 30 µg/l.
At baseline, a total of 54.5% of participants showed functional iron deficiency at a mean hemoglobin of 14.3 g/dl; while, the rate of absolute iron deficiency was 11.8%, at a mean hemoglobin level of 13.4 g/dl. At year 5, proportion of newly diagnosed subjects was 18.5% and 4.8%, respectively. Rate of all-cause mortality was 7.2% (n = 361); while, median follow-up was 10.1 years. After adjustment for hemoglobin and major cardiovascular risk factors, the hazard ratio with 95% confidence interval of the association of iron deficiency with mortality was 1.3 (1.0-1.6; p = 0.023) for the functional definition, and 1.9 (1.3-2.8; p = 0.002) for absolute iron deficiency.
Iron deficiency is very common in the apparently healthy general population and independently associated with all-cause mortality in the mid to long term.
铁缺乏症现在被认为是一种独立于贫血之外的病症。最近,一种新的铁缺乏症功能定义被提出,并在静脉铁补充的随机心血管临床试验中证明了其强大的疗效。在这里,我们根据两种不同的定义,描述铁缺乏症对非贫血普通人群全因死亡率的影响。
哥廷根健康研究是一项基于人群的前瞻性单中心队列研究。5000 名 35 至 74 岁的个体接受了基线和计划在第 5 年进行的随访。所测试的铁缺乏症定义包括(1)功能性铁缺乏症——铁蛋白水平低于 100μg/l,或铁蛋白水平在 100 至 299μg/l 之间且转铁蛋白饱和度低于 20%,以及(2)绝对铁缺乏症——铁蛋白水平低于 30μg/l。
在基线时,共有 54.5%的参与者在平均血红蛋白为 14.3g/dl 时表现出功能性铁缺乏症;而绝对铁缺乏症的发生率为 11.8%,平均血红蛋白水平为 13.4g/dl。在第 5 年,新诊断患者的比例分别为 18.5%和 4.8%。全因死亡率为 7.2%(n=361);中位随访时间为 10.1 年。在校正血红蛋白和主要心血管危险因素后,铁缺乏症与死亡率之间关联的风险比(95%置信区间)为 1.3(1.0-1.6;p=0.023),功能性定义为 1.9(1.3-2.8;p=0.002)。
在明显健康的普通人群中,铁缺乏症非常常见,并且与中期至长期的全因死亡率独立相关。