Odendaal Willem A, Anstey Watkins Jocelyn, Leon Natalie, Goudge Jane, Griffiths Frances, Tomlinson Mark, Daniels Karen
South African Medical Research Council, Health Systems Research Unit, Cape Town, Western Cape, South Africa.
Stellenbosch University, Department of Psychiatry, Cape Town, South Africa.
Cochrane Database Syst Rev. 2020 Mar 26;3(3):CD011942. doi: 10.1002/14651858.CD011942.pub2.
Mobile health (mHealth), refers to healthcare practices supported by mobile devices, such as mobile phones and tablets. Within primary care, health workers often use mobile devices to register clients, track their health, and make decisions about care, as well as to communicate with clients and other health workers. An understanding of how health workers relate to, and experience mHealth, can help in its implementation.
To synthesise qualitative research evidence on health workers' perceptions and experiences of using mHealth technologies to deliver primary healthcare services, and to develop hypotheses about why some technologies are more effective than others.
We searched MEDLINE, Embase, CINAHL, Science Citation Index and Social Sciences Citation Index in January 2018. We searched Global Health in December 2015. We screened the reference lists of included studies and key references and searched seven sources for grey literature (16 February to 5 March 2018). We re-ran the search strategies in February 2020. We screened these records and any studies that we identified as potentially relevant are awaiting classification.
We included studies that used qualitative data collection and analysis methods. We included studies of mHealth programmes that were part of primary healthcare services. These services could be implemented in public or private primary healthcare facilities, community and workplace, or the homes of clients. We included all categories of health workers, as well as those persons who supported the delivery and management of the mHealth programmes. We excluded participants identified as technical staff who developed and maintained the mHealth technology, without otherwise being involved in the programme delivery. We included studies conducted in any country.
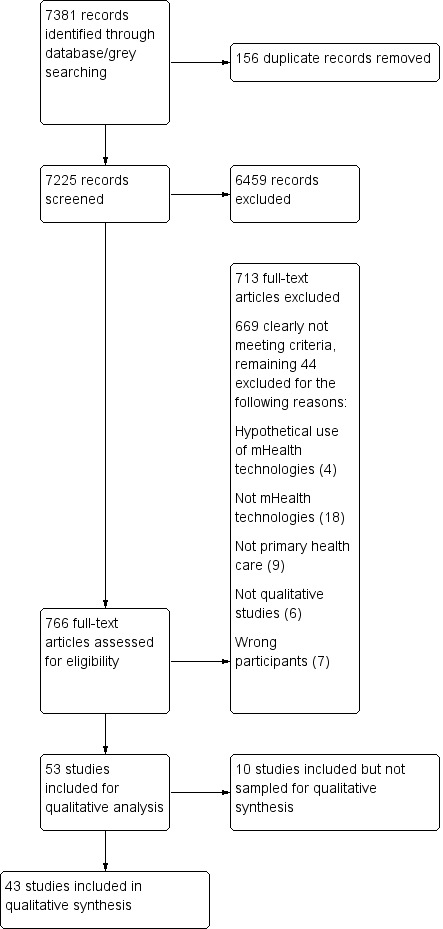
We assessed abstracts, titles and full-text papers according to the inclusion criteria. We found 53 studies that met the inclusion criteria and sampled 43 of these for our analysis. For the 43 sampled studies, we extracted information, such as country, health worker category, and the mHealth technology. We used a thematic analysis process. We used GRADE-CERQual to assess our confidence in the findings.
Most of the 43 included sample studies were from low- or middle-income countries. In many of the studies, the mobile devices had decision support software loaded onto them, which showed the steps the health workers had to follow when they provided health care. Other uses included in-person and/or text message communication, and recording clients' health information. Almost half of the studies looked at health workers' use of mobile devices for mother, child, and newborn health. We have moderate or high confidence in the following findings. mHealth changed how health workers worked with each other: health workers appreciated being more connected to colleagues, and thought that this improved co-ordination and quality of care. However, some described problems when senior colleagues did not respond or responded in anger. Some preferred face-to-face connection with colleagues. Some believed that mHealth improved their reporting, while others compared it to "big brother watching". mHealth changed how health workers delivered care: health workers appreciated how mHealth let them take on new tasks, work flexibly, and reach clients in difficult-to-reach areas. They appreciated mHealth when it improved feedback, speed and workflow, but not when it was slow or time consuming. Some health workers found decision support software useful; others thought it threatened their clinical skills. Most health workers saw mHealth as better than paper, but some preferred paper. Some health workers saw mHealth as creating more work. mHealth led to new forms of engagement and relationships with clients and communities: health workers felt that communicating with clients by mobile phone improved care and their relationships with clients, but felt that some clients needed face-to-face contact. Health workers were aware of the importance of protecting confidential client information when using mobile devices. Some health workers did not mind being contacted by clients outside working hours, while others wanted boundaries. Health workers described how some community members trusted health workers that used mHealth while others were sceptical. Health workers pointed to problems when clients needed to own their own phones. Health workers' use and perceptions of mHealth could be influenced by factors tied to costs, the health worker, the technology, the health system and society, poor network access, and poor access to electricity: some health workers did not mind covering extra costs. Others complained that phone credit was not delivered on time. Health workers who were accustomed to using mobile phones were sometimes more positive towards mHealth. Others with less experience, were sometimes embarrassed about making mistakes in front of clients or worried about job security. Health workers wanted training, technical support, user-friendly devices, and systems that were integrated into existing electronic health systems. The main challenges health workers experienced were poor network connections, access to electricity, and the cost of recharging phones. Other problems included damaged phones. Factors outside the health system also influenced how health workers experienced mHealth, including language, gender, and poverty issues. Health workers felt that their commitment to clients helped them cope with these challenges.
AUTHORS' CONCLUSIONS: Our findings propose a nuanced view about mHealth programmes. The complexities of healthcare delivery and human interactions defy simplistic conclusions on how health workers will perceive and experience their use of mHealth. Perceptions reflect the interplay between the technology, contexts, and human attributes. Detailed descriptions of the programme, implementation processes and contexts, alongside effectiveness studies, will help to unravel this interplay to formulate hypotheses regarding the effectiveness of mHealth.
移动健康(mHealth)是指由移动设备(如手机和平板电脑)支持的医疗保健实践。在初级保健中,卫生工作者经常使用移动设备为客户登记、跟踪其健康状况、做出护理决策,以及与客户和其他卫生工作者进行沟通。了解卫生工作者如何与移动健康相关联以及体验移动健康,有助于其实施。
综合关于卫生工作者对使用移动健康技术提供初级医疗服务的看法和体验的定性研究证据,并就为何某些技术比其他技术更有效提出假设。
我们于2018年1月检索了MEDLINE、Embase、CINAHL、科学引文索引和社会科学引文索引。于2015年12月检索了《全球健康》。我们筛选了纳入研究和关键参考文献的参考文献列表,并于2018年2月16日至3月5日在七个来源中检索灰色文献。我们在2020年2月重新运行了检索策略。我们筛选了这些记录,任何我们确定为可能相关的研究正在等待分类。
我们纳入了使用定性数据收集和分析方法的研究。我们纳入了作为初级医疗服务一部分的移动健康项目的研究。这些服务可以在公共或私人初级医疗保健设施、社区和工作场所或客户家中实施。我们纳入了所有类别的卫生工作者,以及那些支持移动健康项目实施和管理的人员。我们排除了被确定为开发和维护移动健康技术但未以其他方式参与项目实施的技术人员。我们纳入了在任何国家进行的研究。
我们根据纳入标准评估摘要、标题和全文论文。我们发现53项研究符合纳入标准,并从中抽取43项进行分析。对于抽取的43项研究,我们提取了国家、卫生工作者类别和移动健康技术等信息。我们采用了主题分析过程。我们使用GRADE-CERQual评估我们对研究结果的信心。
43项纳入样本研究中的大多数来自低收入或中等收入国家。在许多研究中,移动设备加载了决策支持软件,该软件展示了卫生工作者提供医疗服务时必须遵循的步骤。其他用途包括面对面和/或短信通信,以及记录客户的健康信息。几乎一半的研究关注卫生工作者使用移动设备进行母婴和新生儿健康方面的工作。我们对以下研究结果有中等或高度信心。移动健康改变了卫生工作者之间的工作方式:卫生工作者赞赏与同事之间联系更紧密,并认为这改善了协调和护理质量。然而,一些人描述了上级同事不回应或愤怒回应时出现的问题。一些人更喜欢与同事面对面交流。一些人认为移动健康改善了他们的报告工作,而另一些人则将其比作“老大哥在监视”。移动健康改变了卫生工作者提供护理的方式:卫生工作者赞赏移动健康使他们能够承担新任务、灵活工作,并接触到难以到达地区的客户。当移动健康改善反馈、速度和工作流程时,他们会赞赏,但当它缓慢或耗时的时候则不然。一些卫生工作者发现决策支持软件有用;另一些人则认为它威胁到了他们的临床技能。大多数卫生工作者认为移动健康比纸质方式更好,但也有一些人更喜欢纸质方式。一些卫生工作者认为移动健康带来了更多工作。移动健康导致了与客户和社区互动及关系的新形式:卫生工作者认为通过手机与客户沟通改善了护理以及他们与客户的关系,但觉得一些客户需要面对面接触。卫生工作者意识到在使用移动设备时保护客户机密信息的重要性。一些卫生工作者不介意在工作时间之外被客户联系,而另一些人则希望有界限。卫生工作者描述了一些社区成员信任使用移动健康的卫生工作者,而另一些人则持怀疑态度。卫生工作者指出当客户需要拥有自己的手机时会出现问题。卫生工作者对移动健康的使用和看法可能受到与成本、卫生工作者、技术、卫生系统和社会、网络接入差以及电力供应差相关的因素影响:一些卫生工作者不介意承担额外费用。另一些人抱怨手机话费未按时到账。习惯使用手机的卫生工作者有时对移动健康更积极。其他经验较少的人有时会因在客户面前犯错而感到尴尬或担心工作安全。卫生工作者希望得到培训、技术支持、用户友好的设备以及集成到现有电子健康系统中的系统。卫生工作者遇到的主要挑战是网络连接差、电力供应以及手机充电成本。其他问题包括手机损坏。卫生系统之外的因素也影响了卫生工作者体验移动健康的方式,包括语言、性别和贫困问题。卫生工作者认为他们对客户的承诺帮助他们应对这些挑战。
我们的研究结果对移动健康项目提出了细致入微的观点。医疗服务提供和人际互动的复杂性使得关于卫生工作者如何看待和体验他们对移动健康的使用难以得出简单结论。看法反映了技术、背景和人类属性之间的相互作用。对项目、实施过程和背景的详细描述以及有效性研究,将有助于揭示这种相互作用,以形成关于移动健康有效性的假设。