Rungsakulkij Narongsak, Thewmorakot Siraprapa, Suragul Wikran, Vassanasiri Watoo, Tangtawee Pongsatorn, Muangkaew Paramin, Mingphruedhi Somkit, Aeesoa Suraida
Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand.
World J Gastrointest Surg. 2020 Mar 27;12(3):93-103. doi: 10.4240/wjgs.v12.i3.93.
Laparoscopic cholecystectomy (LC) is a minimally invasive procedure, often performed by surgical residents (SRs). Fluorescence cholangiography (FC) enables real-time identification of biliary anatomy.
To investigate the benefit of FC for enhancing SRs' identification skills.
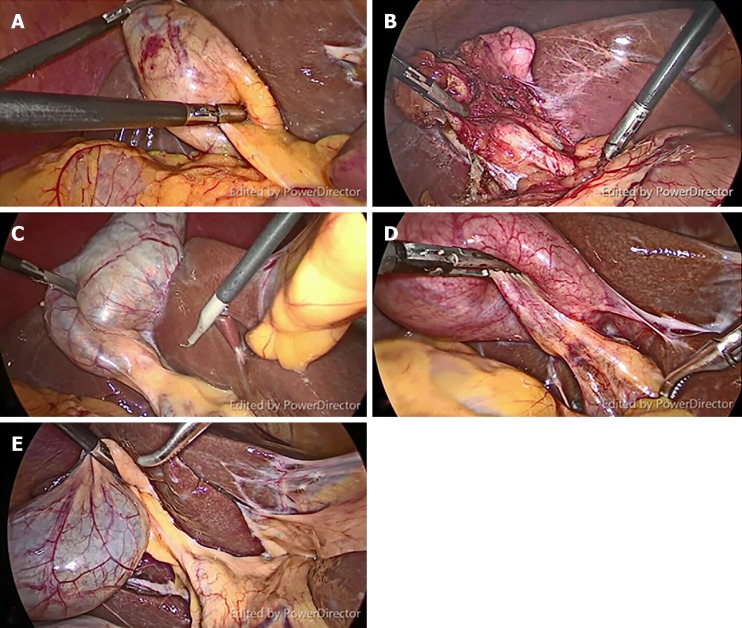
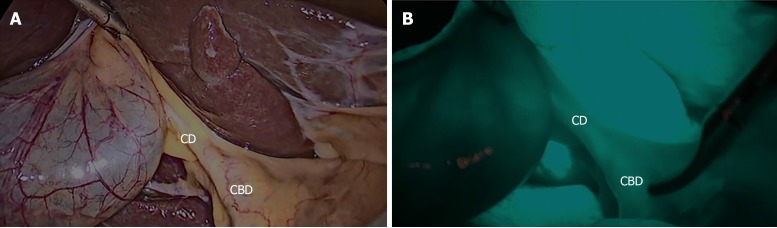
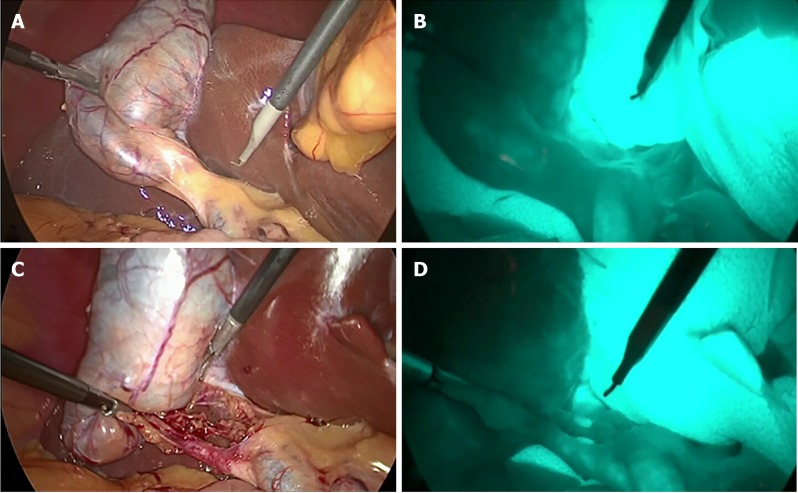
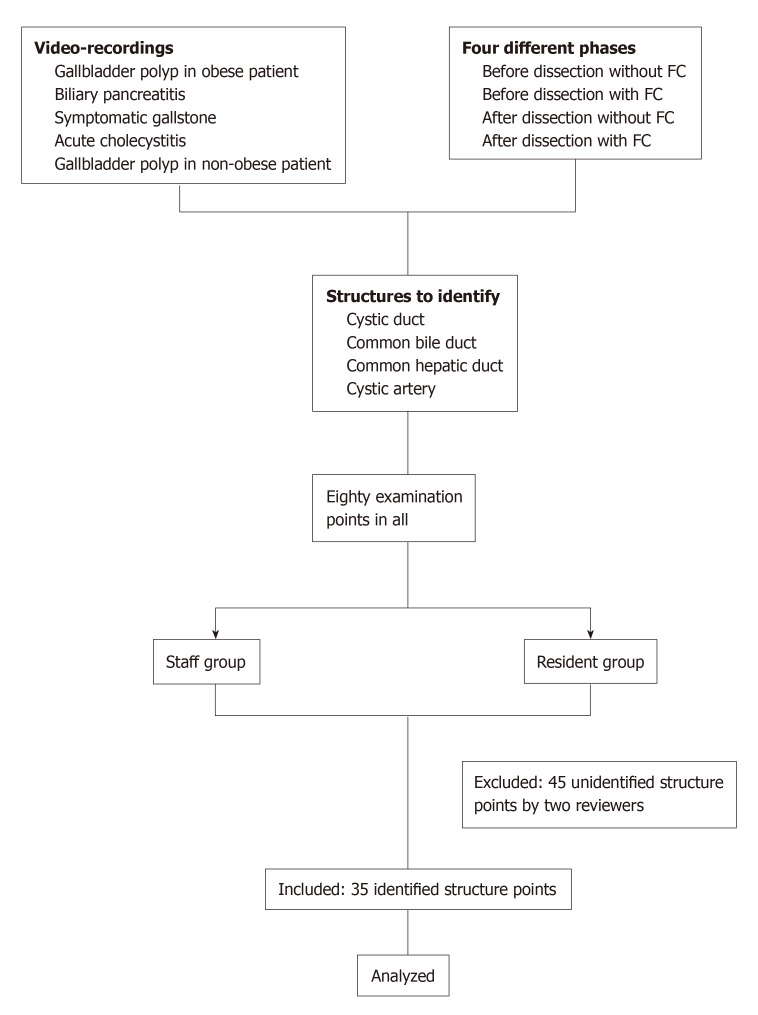
Prospective data was collected from January 2018 to June 2018 at our hospital. The study cohorts were the SRs (study group, = 15) and the surgical staff (SS; control group, = 9). Participants were assigned to watch videos of LCs with FC from five different patients who had gallbladder disease, and identify structures in the video clips (including cystic duct, common bile duct, common hepatic duct, and cystic artery), first without FC, and then with FC.
In the without-FC phase, the overall misidentification rate by SRs (21.7%) was greater than that of the SS (11.8%; = 0.018), However, in the FC phase, the two groups did not significantly differ in misidentification rates (23.3% 23.3%, = 0.99). Paired-structure analysis of the without-FC and with-FC phases for the SR group found a significantly higher misidentification rate in the without-FC phase than the with-FC phase (21.9% 10.9%; < 0.01). However, misidentification rates in the with-FC phase did not significantly differ between SRs and SS.
FC enhanced identification skills of inexperienced surgeons during LC compared with conventional training. Combined with simulation-based video training, FC is a promising tool for enhancing technical and decision skills of trainees and inexperienced surgeons.
腹腔镜胆囊切除术(LC)是一种微创手术,通常由外科住院医师(SRs)进行。荧光胆管造影(FC)能够实时识别胆道解剖结构。
探讨FC对提高SRs识别技能的益处。
于2018年1月至2018年6月在我院收集前瞻性数据。研究队列包括SRs(研究组,n = 15)和手术人员(SS;对照组,n = 9)。参与者被分配观看5例患有胆囊疾病患者的LC伴FC的视频,并识别视频片段中的结构(包括胆囊管、胆总管、肝总管和胆囊动脉),先是在无FC的情况下,然后是在有FC的情况下。
在无FC阶段,SRs的总体错误识别率(21.7%)高于SS(11.8%;P = 0.018)。然而,在FC阶段,两组的错误识别率无显著差异(23.3%对23.3%,P = 0.99)。对SR组无FC和有FC阶段进行配对结构分析发现,无FC阶段的错误识别率显著高于有FC阶段(21.9%对10.9%;P < 0.01)。然而,有FC阶段SRs和SS的错误识别率无显著差异。
与传统培训相比,FC在LC期间提高了经验不足的外科医生的识别技能。结合基于模拟的视频培训,FC是提高学员和经验不足的外科医生技术和决策技能的一种有前景的工具。