Choi Young Hoon, Lee Sang Hyub, You Min Su, Shin Bang Sup, Paik Woo Hyun, Ryu Ji Kon, Kim Yong-Tae, Kwon Wooil, Jang Jin-Young, Kim Sun-Whe
Department of Internal Medicine and Liver Research Institute, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Division of Gastroenterology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Gut Liver. 2021 Mar 15;15(2):315-323. doi: 10.5009/gnl19182.
BACKGROUND/AIMS: There has been growing evidence on the utility of neoadjuvant FOLFIRINOX in borderline resectable (BR) or locally advanced (LA) pancreatic cancer. However, factors predicting survival in these patients remain to be identified, and we aimed to identify these prognostic factors.
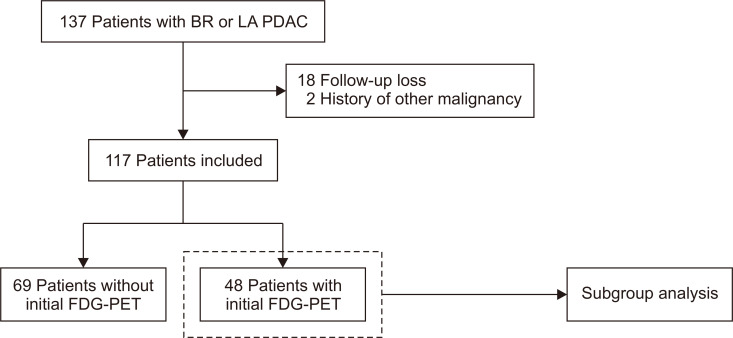
Between January 2013 and April 2017, patients with BR or LA pancreatic cancer who received FOLFIRINOX as their initial treatment were identified. Demographic data and clinical outcomes, including the chemotherapy response, conversion to resection, and survival, were reviewed.
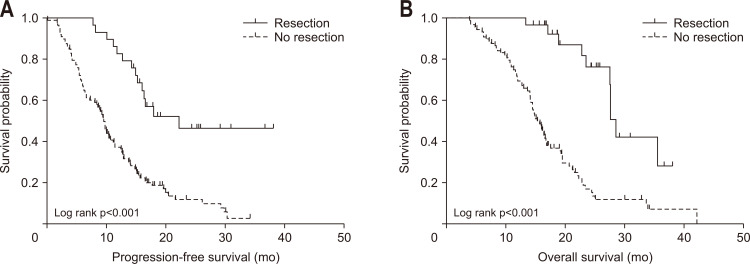
A total of 117 patients with BR (n=39) or LA (n=78) pancreatic cancer were included. Of these patients, 29 (24.8%) underwent curative surgery, and R0 resection was achieved in 21 patients (72.4%). The median progression-free survival and overall survival time of all patients were 11.6 and 19.0 months, respectively. In resected patients, the median relapse-free survival and overall survival times were 14.8 and 28.6 months, respectively. In the multivariate Cox model, the lowest level of serum carbohydrate antigen 19-9 (CA 19-9) and resection after FOLFIRINOX were independent factors for improved overall survival. In the subgroup analysis of patients with initial F-fluorodeoxyglucose-positron emission tomography (FDG-PET) images, the maximum standardized uptake value (SUVmax) of the pancreatic mass was also shown as an independent factor for improved overall survival.
In patients with BR or LA pancreatic cancer, FOLFIRINOX is a valuable neoadjuvant treatment that enables curative surgery in approximately one-quarter of patients and significantly improves overall survival. In these patients, the prognosis can be estimated using the lowest level of serum CA 19-9, operative status, and initial FDG-PET SUVmax.
背景/目的:新辅助FOLFIRINOX方案在可切除边缘(BR)或局部进展期(LA)胰腺癌中的应用价值已有越来越多的证据。然而,这些患者生存的预测因素仍有待确定,我们旨在识别这些预后因素。
确定2013年1月至2017年4月期间接受FOLFIRINOX作为初始治疗的BR或LA胰腺癌患者。回顾人口统计学数据和临床结局,包括化疗反应、转为手术切除和生存情况。
共纳入117例BR(n = 39)或LA(n = 78)胰腺癌患者。其中,29例(24.8%)接受了根治性手术,21例(72.4%)实现了R0切除。所有患者的中位无进展生存期和总生存期分别为11.6个月和19.0个月。在接受手术切除的患者中,中位无复发生存期和总生存期分别为14.8个月和28.6个月。在多变量Cox模型中,血清糖类抗原19-9(CA 19-9)最低水平和FOLFIRINOX治疗后切除是总生存期改善的独立因素。在初始F-氟脱氧葡萄糖正电子发射断层扫描(FDG-PET)图像患者的亚组分析中,胰腺肿块最大标准化摄取值(SUVmax)也显示为总生存期改善的独立因素。
在BR或LA胰腺癌患者中,FOLFIRINOX是一种有价值的新辅助治疗方法,约四分之一的患者能够接受根治性手术,并显著提高总生存期。在这些患者中,可使用血清CA 19-9最低水平、手术状态和初始FDG-PET SUVmax来评估预后。