Department of Infectious Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Zambart, University of Zambia School of Medicine, Lusaka, Zambia.
PLoS Med. 2020 Apr 2;17(4):e1003067. doi: 10.1371/journal.pmed.1003067. eCollection 2020 Apr.
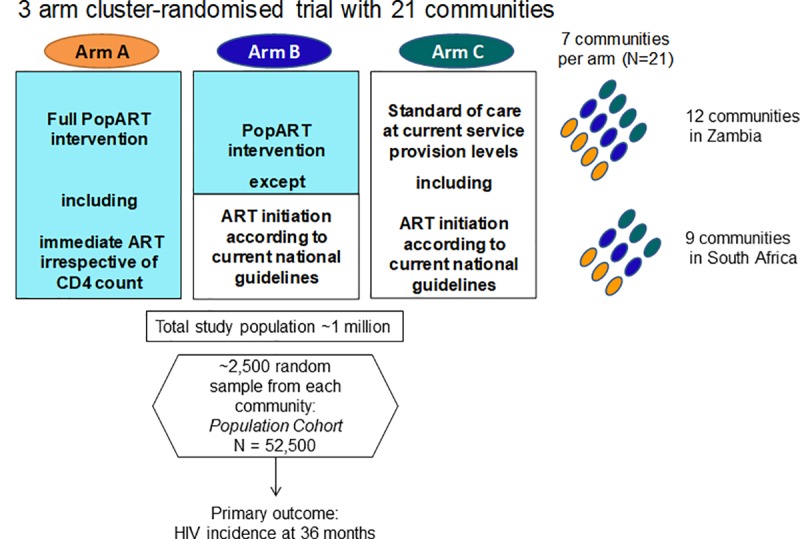
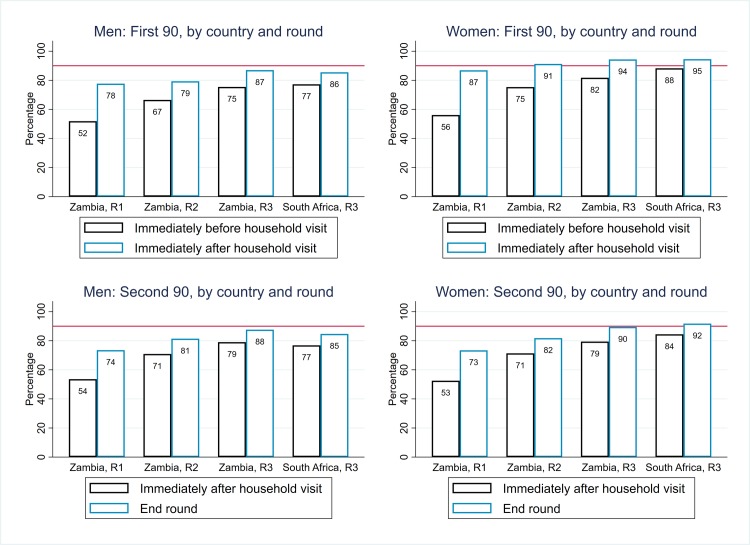
In 2014, the Joint United Nations Programme on HIV/AIDS (UNAIDS) set the 90-90-90 targets: that 90% of people living with HIV know their HIV status, that 90% of those who know their HIV-positive status are on antiretroviral therapy (ART), and that 90% of those on treatment are virally suppressed. The aim was to reach these targets by 2020. We assessed the feasibility of achieving the first two targets, and the corresponding 81% ART coverage target, as part of the HIV Prevention Trials Network (HPTN) 071 Population Effects of Antiretroviral Therapy to Reduce HIV Transmission (PopART) community-randomized trial.
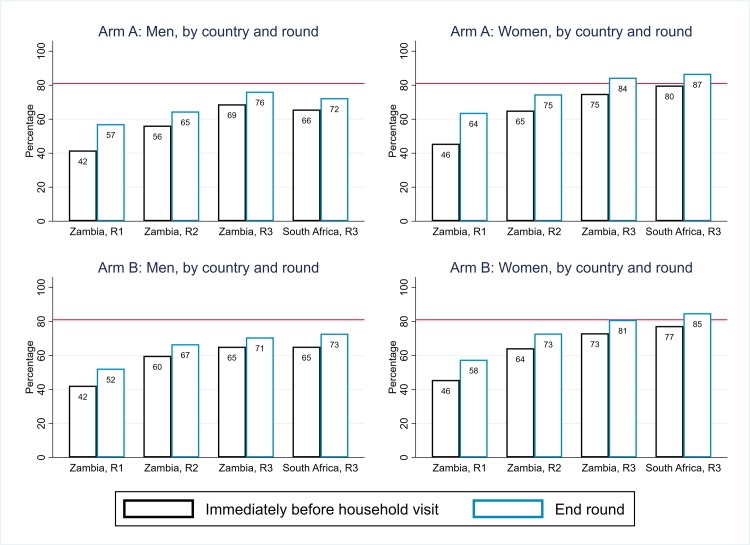
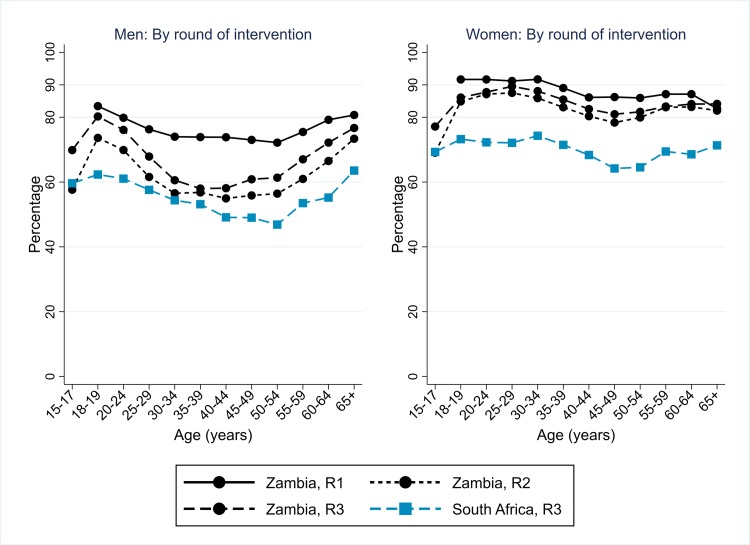
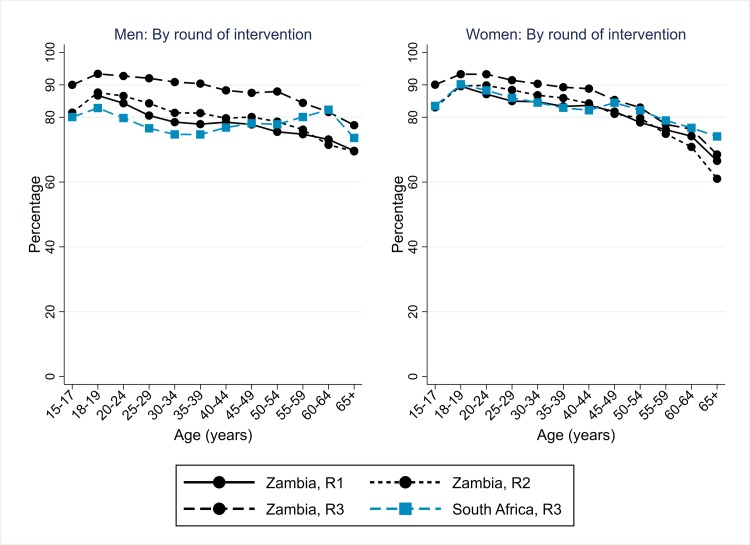
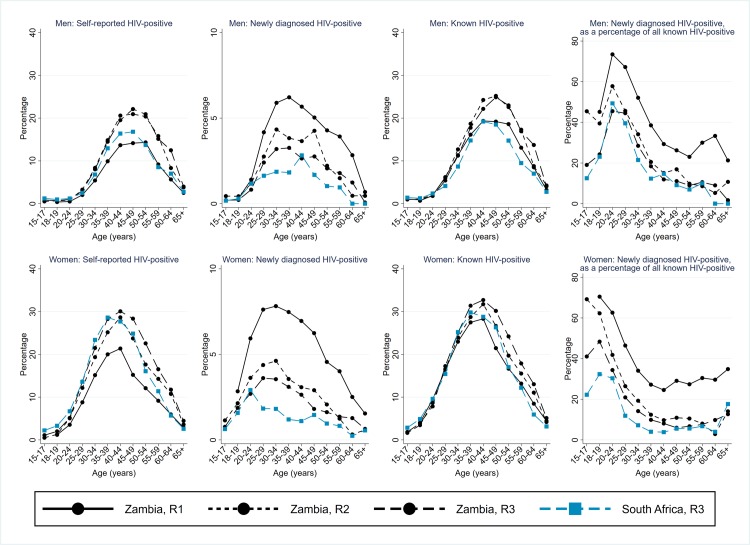
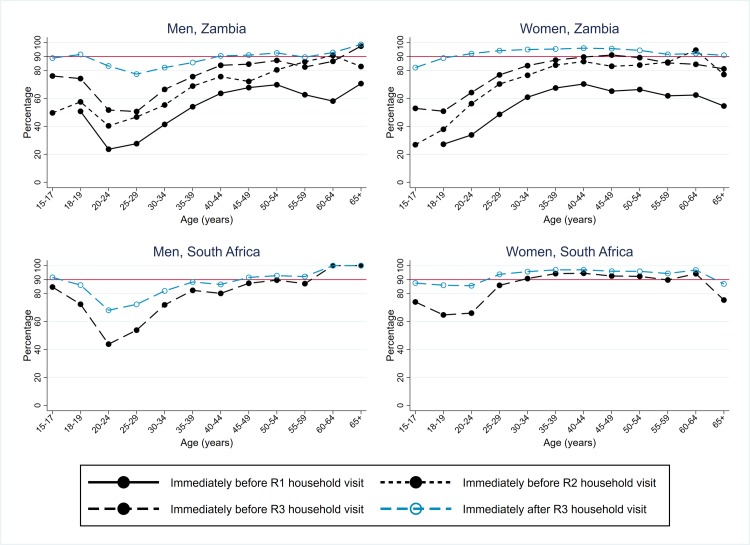
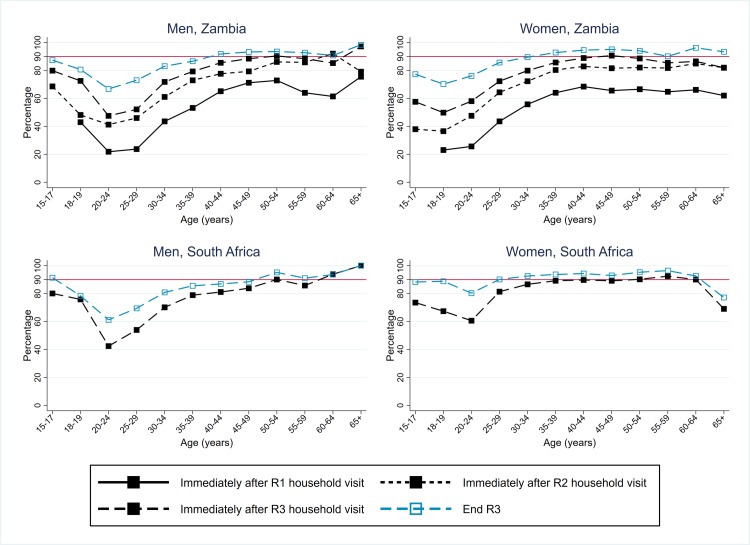
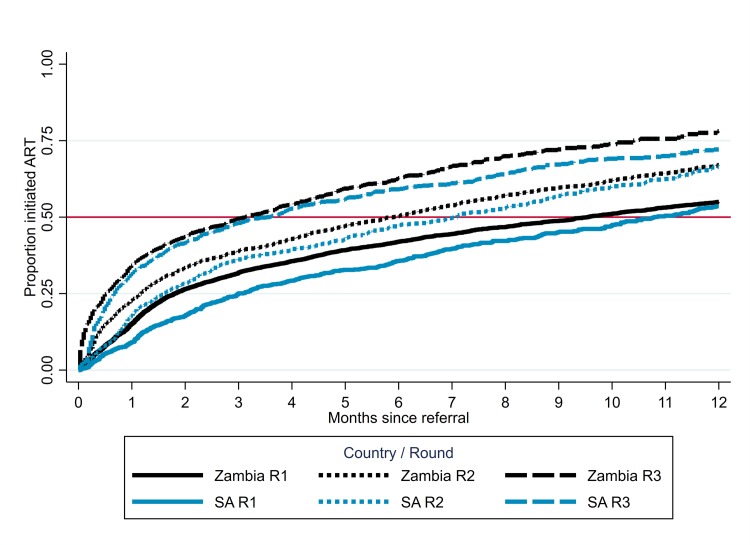
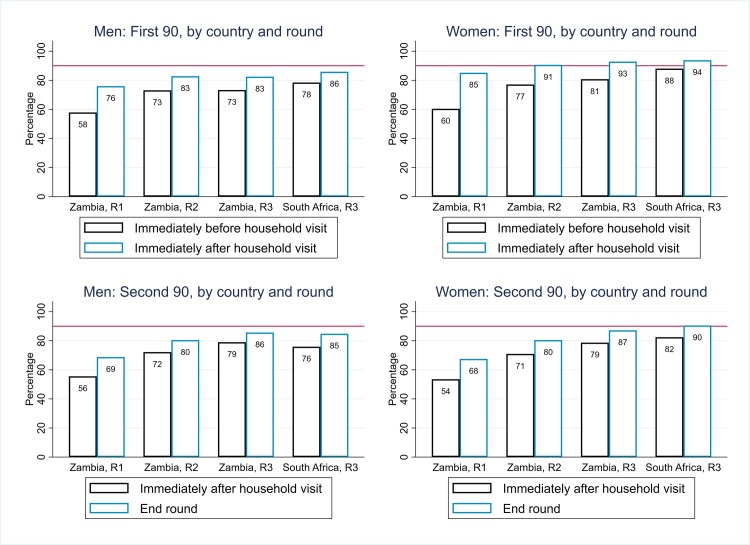
The study population was individuals aged ≥15 years living in 14 urban and peri-urban "PopART intervention" communities in Zambia and South Africa (SA), with a total population of approximately 600,000 and approximately 15% adult HIV prevalence. Community HIV care providers (CHiPs) delivered the PopART intervention during 2014-2017. This was a combination HIV prevention package including universal home-based HIV testing, referral of HIV-positive individuals to government HIV clinic services that offered universal ART (Arm A) or ART according to national guidelines (Arm B), and revisits to HIV-positive individuals to support linkage to HIV care and retention on ART. The intervention was delivered in 3 "rounds," each about 15 months long, during which CHiPs visited all households and aimed to contact all individuals aged ≥15 years at least once. In Arm A in Round 3 (R3), 67% (41,332/61,402) of men and 86% (56,345/65,896) of women in Zambia and 56% (17,813/32,095) of men and 71% (24,461/34,514) of women in SA participated in the intervention, among 193,907 residents aged ≥15 years. Following participation, HIV status was known by 90% of men and women in Zambia and by 78% of men and 85% of women in SA. The median time from CHiP referral of HIV-positive individuals to ART initiation was approximately 3 months. By the end of R3, an estimated 95% of HIV-positive women and 85% of HIV-positive men knew their HIV status, and among these individuals, approximately 90% of women and approximately 85% of men were on ART. ART coverage among all HIV-positive individuals was approximately 85% in women and approximately 75% in men, up from about 45% at the start of the study. ART coverage was lowest among men aged 18 to 34 and women aged 15 to 24 years, and among mobile individuals/in-migrants. Findings from Arm B were similar. The main limitations to our study were that estimates of testing and treatment coverage among men relied on considerable extrapolation because, in each round, approximately one-third of men did not participate in the PopART intervention; that our findings are for a service delivery model that was relatively intensive; and that we did not have comparable data from the 7 "standard-of-care" (Arm C) communities.
Our study showed that very high HIV testing and treatment coverage can be achieved through persistent delivery of universal testing, facilitated linkage to HIV care, and universal treatment services. The ART coverage target of 81% was achieved overall, after 4 years of delivery of the PopART intervention, though important gaps remained among men and young people. Our findings are consistent with previously reported findings from southern and east Africa, extending their generalisability to urban settings with high rates of in-migration and mobility and to Zambia and SA.
ClinicalTrials.gov NCT01900977.
2014 年,联合国艾滋病规划署(UNAIDS)制定了 90-90-90 目标:即 90%的艾滋病毒感染者知晓其艾滋病毒状况,90%知晓自身状况的感染者接受抗逆转录病毒治疗(ART),90%接受治疗的感染者病毒得到抑制。目标是到 2020 年实现这些目标。我们评估了实现前两个目标的可行性,以及作为 HIV 预防试验网络(HPTN)071 人群效应抗逆转录病毒治疗减少 HIV 传播(PopART)社区随机试验的一部分,实现相应的 81%的 ART 覆盖率目标的可行性。
研究人群为年龄≥15 岁的个体,居住在赞比亚和南非(SA)的 14 个城市和城郊“PopART 干预”社区,总人数约为 60 万,成人 HIV 感染率约为 15%。社区 HIV 护理提供者(CHiPs)在 2014-2017 年期间提供了 PopART 干预。这是一个结合了通用家庭 HIV 检测、将 HIV 阳性个体转介到政府 HIV 诊所服务的 HIV 预防方案,这些诊所提供了普遍的 ART(Arm A)或根据国家指南提供的 ART(Arm B),并对 HIV 阳性个体进行回访,以支持他们与 HIV 护理的联系,并保持对 ART 的治疗。该干预在三轮中进行,每轮约 15 个月,在此期间,CHiPs 访问了所有家庭,并旨在至少与所有≥15 岁的人联系一次。在第三轮(R3)中,赞比亚的男性参与者中 67%(41,332/61,402)和女性参与者中 86%(56,345/65,896),南非的男性参与者中 56%(17,813/32,095)和女性参与者中 71%(24,461/34,514)参加了干预,在 193,907 名≥15 岁的居民中。参与后,赞比亚的男性和女性中 90%和 78%的人知道自己的 HIV 状况,SA 的男性和女性中 85%和 85%的人知道自己的 HIV 状况。从 CHiP 转介 HIV 阳性个体到开始接受 ART 的时间中位数约为 3 个月。到 R3 结束时,估计有 95%的 HIV 阳性女性和 85%的 HIV 阳性男性知道自己的 HIV 状况,在这些人中,约 90%的女性和约 85%的男性正在接受 ART。所有 HIV 阳性个体中,ART 覆盖率约为女性的 85%,男性的 75%,高于研究开始时的约 45%。ART 覆盖率在 18 至 34 岁的男性和 15 至 24 岁的女性以及流动人员/移民中最低。Arm B 的结果类似。我们研究的主要限制是,对男性检测和治疗覆盖率的估计依赖于大量的推断,因为在每一轮中,大约三分之一的男性没有参与 PopART 干预;我们的研究结果是基于相对密集的服务提供模式;我们没有来自 7 个“标准护理”(Arm C)社区的可比数据。
我们的研究表明,通过持续提供通用检测、促进与 HIV 护理的联系和普遍的治疗服务,可以实现非常高的 HIV 检测和治疗覆盖率。在实施 PopART 干预 4 年后,实现了 81%的 ART 覆盖率目标,尽管男性和年轻人中仍存在重要差距。我们的研究结果与以前在南部和东部非洲的报告结果一致,将其普遍性扩展到高移民和流动率的城市环境以及赞比亚和南非。
ClinicalTrials.gov NCT01900977。