Section for cervical cancer screening, Cancer Registry of Norway, Oslo, Norway.
Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, NY, USA.
Br J Cancer. 2020 May;122(11):1715-1723. doi: 10.1038/s41416-020-0790-1. Epub 2020 Apr 3.
HPV16/18 detection may improve cervical cancer risk stratification and better guide which HPV-positive women warrant immediate colposcopy/biopsy. We estimated risks of cervical precancer and cancer by HPV genotype and cytology during the implementation phase of primary HPV testing in Norway.
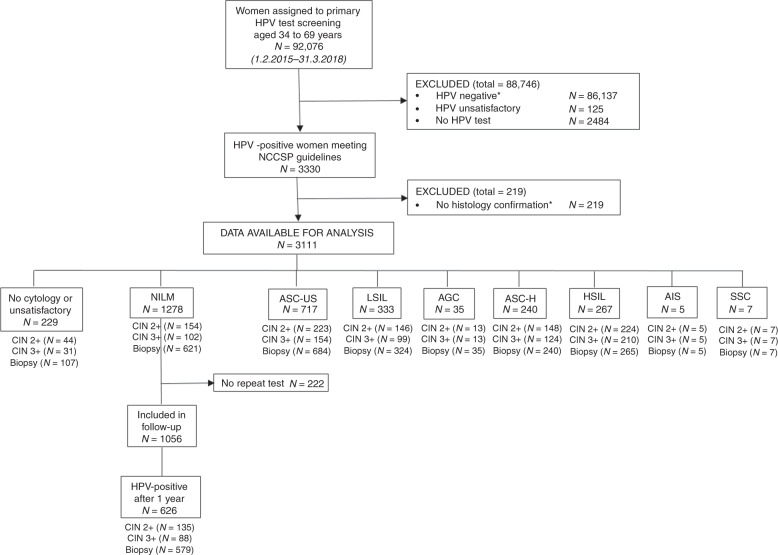
A total of 3111 women, aged 34-69 years, testing HPV-positive at baseline and undergoing cytology testing from February 2015 to April 2018 had data available for analysis. Risk estimates with 95% confidence intervals (95%CIs) of cervical intraepithelial neoplasia grade 3 or more severe (CIN3+) were estimated for cytology results and HPV genotypes (HPV16, HPV18, and other high-risk HPV).
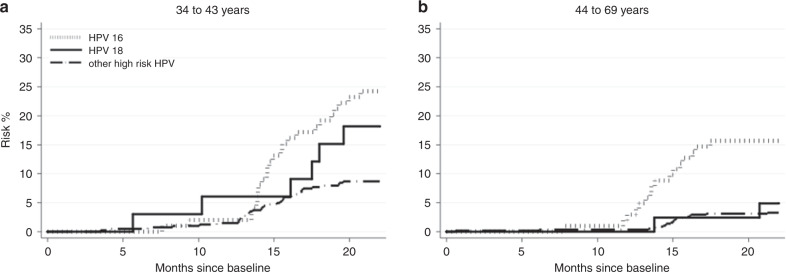
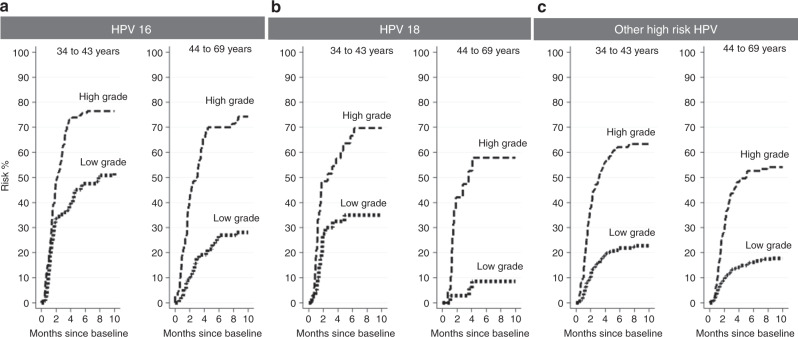
CIN3+ risks were higher for HPV16/18 than other high-risk HPV genotypes. Among women with any cytologic abnormality [atypical squamous cells of undetermined significance or worse], immediate risks were 57.8% (95%CI = 53.0-62.6%) for HPV16, 40.2% (95%CI = 32.3-49.2%) for HPV18, and 31.4% (95%CI = 28.7-34.3%) for other high-risk HPV. Among those with normal cytology, CIN3+ risks were 19.9% (95%CI = 15.0-26.1%) for HPV16 positives, 10.8% (95%CI = 5.6-20.5%) for HPV18 positives, and 5.5% (95%CI = 4.2-7.1%) for other high-risk HPV.
The benefits and harms of managing women based on HPV positivity and cytology results can be better balanced by inclusion of HPV genotyping in screening and choosing more conservative management for other high-risk HPV compared to HPV16/18.
HPV16/18 检测可改善宫颈癌风险分层,并更好地指导哪些 HPV 阳性妇女需要立即行阴道镜检查/活检。我们在挪威 HPV 初筛实施阶段,根据 HPV 基因型和细胞学检测结果估计了宫颈癌前病变和癌症的风险。
共有 3111 名年龄在 34-69 岁的妇女,在基线时 HPV 阳性,并于 2015 年 2 月至 2018 年 4 月期间接受细胞学检查,这些妇女的数据可用于分析。对细胞学结果和 HPV 基因型(HPV16、HPV18 和其他高危型 HPV)为 HPV16/18 和其他高危型 HPV 的宫颈癌上皮内瘤变 3 级或更高级别(CIN3+)的风险估计值,使用 95%置信区间(95%CI)进行估计。
HPV16/18 比其他高危型 HPV 基因型的 CIN3+风险更高。在任何细胞学异常(非典型鳞状细胞意义不明确或更严重)的妇女中,HPV16 阳性者的即刻风险为 57.8%(95%CI=53.0-62.6%),HPV18 阳性者为 40.2%(95%CI=32.3-49.2%),其他高危型 HPV 阳性者为 31.4%(95%CI=28.7-34.3%)。在细胞学正常的妇女中,HPV16 阳性者的 CIN3+风险为 19.9%(95%CI=15.0-26.1%),HPV18 阳性者为 10.8%(95%CI=5.6-20.5%),其他高危型 HPV 阳性者为 5.5%(95%CI=4.2-7.1%)。
通过 HPV 基因分型纳入筛查,并与 HPV16/18 相比,对其他高危型 HPV 选择更为保守的管理,可以更好地平衡基于 HPV 阳性和细胞学结果管理妇女的获益和危害。